Assessing DFID’s results in nutrition
Score summary
The Department for International Development (DFID) surpassed its goal of reaching 50 million people with nutrition services between 2015 and 2020. The result is valid but misses other important achievements of the department, including building global and national commitments to reduce undernutrition. DFID was successful in reaching many of the most vulnerable women and children, but could have done better by strengthening data systems and investing more in the development of local delivery capacity. The UK aid nutrition portfolio is making significant contributions to reducing malnutrition but could increase its impact by expanding work on healthy diets, and promoting the increased convergence of different programmes on the most vulnerable communities.
Malnutrition is a major cause of preventable deaths in all countries and constrains social and economic development. The Department for International Development (DFID), which has now been merged into the Foreign, Commonwealth and Development Office (FCDO), played a leading role in advocating for nutrition to be a priority. It helped to strengthen political leadership and commitments on reducing undernutrition at both the global and national levels. The Government’s commitment to reach 50 million people with nutrition services between 2015 and 2020 was surpassed early. The methodology used to calculate these results is robust, and helped DFID advisers to understand better the importance of high-impact, multi-sector nutrition programming. However, measurement inaccuracies and inconsistencies across DFID’s country offices highlight the difficulty of applying complex results methodologies in practice. Despite improvements, the UK’s nutrition results are still overly focused on reporting outputs, and it is difficult to tell whether individuals have received support from several different sectors to tackle malnutrition.
Those targeted by DFID’s nutrition programmes – women of childbearing age, adolescent girls and children under five – are some of the world’s most vulnerable to undernutrition. DFID’s ability to work within highly constrained environments, including crisis contexts, to ensure that its nutrition programmes reached these target groups was impressive. Evidence of reaching acutely malnourished children in climate-affected and food-insecure regions demonstrated the department’s capacity to deliver life-saving nutrition services to some of the most vulnerable citizens. However, DFID did not consistently reach the most marginalised within its target groups, including the chronically ill, and did not always fully understand their needs. Weak national data systems, as well as the increasing burden placed on volunteers who often deliver nutrition services, continue to be major challenges.
By championing a multi-sector approach, which addresses the underlying as well as the direct causes of undernutrition, DFID’s programming aligns with the evidence on “what works”. Although most countries are not on track to meet global nutrition goals, many of DFID’s target countries have seen long-term decreases in stunting. DFID’s programmes have made positive contributions towards this trend, as well as influencing additional political and financial commitments to nutrition. Future impact on nutrition can be enhanced through working with FCDO’s partners to strengthen the portfolio’s approach to working across different sectors, including on nutritious food systems, and emphasising the convergence of different interventions on the most vulnerable.
| Individual question scores | |
|---|---|
| Question 1 Effectiveness: How valid are DFID’s reported nutrition results? |  |
| Question 2 Equity: Are DFID interventions reaching the most vulnerable and hard-to-reach women and children? | |
| Question 3 Impact: To what extent is DFID helping to reduce malnutrition? | |
Executive summary
“We know that if a child is not given the right foods, they will be stunted – they will have weak bodies, the child will be a slow learner.”
“The children should be given kapenta, bananas, boiled eggs, soya bean, groundnuts, milk, meat and vegetables. So that the children can have nutrients. But we don’t have such food or money to buy such food.”
“The parent should eat food important for the child’s growth such as fish, vegetables, so that the child can have nutrients. But [the foods] are very difficult to source for poor people like us.”
Focus group participants, Sioma District, Zambia
Good nutrition is a fundamental prerequisite for the development of an individual and a country. It is essential for a healthy immune system and cognitive, motor and emotional development. Within the context of the COVID-19 pandemic, the need for good nutrition is further heightened: nutritional well-being can help protect the most vulnerable from the risk of severe illnesses. However, the burden of malnutrition remains alarmingly high and poses a significant threat to livelihoods, communities and economies. One in nine people in the world are hungry and around 45% of all deaths among children under five are linked to undernutrition. Now COVID-19 and the associated response are predicted to cause a huge increase in the number of people facing hunger and malnutrition.
In recent years, recognition of the benefits of investing in nutrition has increased and significant strides have been made to ensure that tackling undernutrition is a global priority. Nutrition interventions are consistently identified as highly cost-effective. The UK’s Department for International Development (DFID) and its nutrition policy team have been at the forefront of the increased focus on reducing undernutrition. In 2013, the UK held the first Nutrition for Growth Summit, culminating in the signing of the Global Nutrition for Growth Compact by 94 stakeholders, including development partners, businesses, scientific organisations and civil society groups. In 2015, the UK’s commitment to eradicate hunger and prevent undernutrition was highlighted through the government’s pledge to reach 50 million people, with a particular focus on women and children, with its nutrition services by 2020. Since this commitment, DFID has published its nutrition results, detailing the number of women of childbearing age, adolescent girls and children under five reached by its programmes.
The causes of maternal and child undernutrition are complex. Undernutrition is the immediate consequence of an inadequate diet and disease. But it is also related to underlying problems including food insecurity, poor sanitation and hygiene and inadequate health services, as well as wider factors related to poverty, climate change and conflict. Tackling the problem effectively and sustainably therefore requires a combined, multi-sector approach. The literature recommends ‘nutrition-specific’ health interventions to address the direct causes of malnutrition (including micronutrient supplementation, breastfeeding advice and treatment for acute malnutrition). It also recommends ‘nutrition-sensitive’ approaches, which involve tailoring and/or targeting other sector programmes (such as water, sanitation and hygiene (WASH), education, social protection and agriculture) to help address the underlying causes of malnutrition. DFID has encouraged an approach whereby these different interventions ‘converge’ on groups vulnerable to undernutrition, to help maximise their impact. The literature also recognises that achieving this approach is only possible if high-level political commitment is combined with strong technical capacities and if development partners align their actions with government-led plans. Technical assistance and advocacy work have therefore been further important elements of DFID’s work.
This review assesses the nutrition results claimed. It examines the methodology used to calculate these results and interrogates the validity of the reported global figure. It also considers how meaningful these results are through the lens of whether the nutrition programmes are meeting their objectives. Understanding whether the programmes reached and met the needs of the most vulnerable and marginalised is another central aspect of the review. Finally, the review judges the longer-term impact of DFID’s approach on undernutrition. This is based upon DFID’s use of evidence, the contributions of its technical assistance and advocacy work, and programme impact.
Overall, ICAI finds that DFID has made important advances in response to ICAI’s previous nutrition review, published in 2014, including significant progress on improving its nutrition results methodology, country programme implementation and national systems strengthening. Given that DFID only started scaling up its work on nutrition in 2013, these achievements are impressive. However, based on ICAI’s recommendations from 2014, progress should have been more rapid in the interrelated areas of targeting the most vulnerable mothers and children, and strengthening national data systems.
Effectiveness: How valid are DFID’s reported nutrition results?
Reported nutrition results have been based on the number of women of childbearing age, adolescent girls, and children under five reached through DFID’s nutrition interventions. The methodology used to calculate these results has been closely aligned with evidence of “what works”, since it encourages targeted interventions that combine nutrition-specific and nutrition-sensitive services (classified by DFID’s methodology as high-intensity interventions).
The methodology has provided a useful tool for DFID country offices to scrutinise the effectiveness of their nutrition programmes. The inclusion of the intensity categorisation enabled DFID advisers to explore how to achieve the convergence of a range of nutrition services that address the direct and indirect causes of undernutrition. However, the results methodology did not capture DFID’s wider advocacy and technical assistance work. ICAI found evidence that DFID secured political commitments and strengthened national systems to combat undernutrition, but these achievements have not been reflected in its results framework.
DFID reported that it reached 50.6 million women, children under five and adolescent girls through its nutrition programmes between April 2015 and the end of March 2019, mostly through what it defined as medium-intensity reach. The department pursued a cautious approach to calculating its results and acted to revise these where discrepancies were discovered. The reported results are broadly valid. However, ICAI found that reporting against the nutrition results methodology was complex and a resource-intensive exercise for staff, and that this led to some inaccuracies and inconsistencies across individual programmes. Reliance on poor-quality programming, and especially national data systems, presented a significant challenge in reporting results.
The review includes a sample of 20 nutrition programmes, 18 of which contributed to the overall nutrition results. Most of these programmes have been judged by ICAI to be effective in achieving their immediate objectives, based on nutrition output and outcome targets. Programmes are most successful when there are efforts to strengthen the political and technical coordination of services, secure political commitments to nutrition and strengthen local delivery capacity.
DFID met its reach target and pioneered a new results methodology, and most of its nutrition programmes have been delivering against their immediate objectives. The accuracy of programme results and the measurement of their outcomes are, however, areas for future improvement. ICAI has therefore scored the effectiveness of the approach as green-amber.
Equity: Are DFID interventions reaching the most vulnerable and hard-to-reach women and children?
The UK’s Global Nutrition Position Paper reaffirms UK aid’s commitment to ’leave no one behind’ and reach the most vulnerable, excluded and disadvantaged people. The most vulnerable to undernutrition are children, especially during the first 1,000 days of life, as well as women of childbearing age and adolescent girls. Support to these groups will deliver the most benefit. DFID’s interventions to date have demonstrated impressive results in reaching these groups, including treating children with acute malnutrition within crisis contexts.
Good practice in targeting nutrition interventions involves a combination of geographic targeting and targeting households with vulnerable groups. DFID’s nutrition programmes have targeted countries (and regions within countries) with a high burden of undernutrition. DFID reported that 85% of its nutrition results have come from countries categorised as ‘highly fragile’ or ‘fragile’, where stunting and wasting tends to be most acute. Sixteen out of the 55 countries classified by the Integrated Food Security Classification as having the worst food crises contributed to the results (from 23 countries with bilateral nutrition programmes).
Through its nutrition portfolio, the UK has been working within challenging environments facing extreme poverty, drought and conflict, where the capacity to identify, target and reach the poorest households is limited. However, ICAI was impressed with DFID’s ability in many cases to navigate these obstacles, including by building on and strengthening existing community structures and resources such as ward committees and health volunteers.
However, ICAI found that DFID’s interventions did not always reach the most marginalised within the target groups, for example households headed by a disabled person, migrant women, and those in the remotest communities, nor did they always monitor their take-up of services. ICAI also found insufficient understanding within DFID of who the most vulnerable are and how to reach them, due to a lack of detailed guidance, sharing of lessons learnt and targeted citizen consultation.
The achievement of reaching vulnerable women and children through nutrition programmes in such challenging contexts is impressive. However, a lack of disaggregated targets, weak data systems, and limits to the capacity of volunteers mean that there is room for improvement in reaching the most marginalised. ICAI has scored DFID’s work in this area as green-amber.
Impact: To what extent is DFID helping to reduce malnutrition?
By committing to a comprehensive approach that targets both the direct and the underlying causes of undernutrition, DFID’s nutrition strategy has been strongly evidence-based with the potential to be highly impactful. ICAI found that DFID has been considered a strong global leader in nutrition and has played an important role in increasing the international focus on undernutrition. The UK convened international events and supported the development of indicators for global nutrition targets. At the national level, DFID strengthened political leadership and helped to increase financial commitments to nutrition. In Zambia, Ethiopia and Nigeria, ICAI found impressive examples where DFID’s advocacy and technical assistance work contributed to the longer-term integration of nutrition within government services and programmes, and particularly health care. External stakeholders observed that further work is needed to promote greater cross-government cooperation and investment in nutrition from different sectors.
While most countries are not on track to meet the global nutrition targets set for 2025, or the Sustainable Development Goal of ending malnutrition by 2030, many target countries are experiencing long-term decreases in stunting. DFID’s programmes have made positive contributions to this trend. In the most extreme contexts, such as Somalia, the Democratic Republic of Congo and Northern Nigeria, they helped to prevent the situation from worsening, through treating large numbers of children suffering from acute malnutrition.
Programme impacts on undernutrition are nonetheless not as great as anticipated, and robust evaluations helped DFID to learn critical lessons. These include the importance of increasing population coverage, ensuring convergence of services (for example nutrition and WASH) on the most vulnerable communities, and addressing the underlying drivers of malnutrition more comprehensively. For example, DFID has made some progress in improving the contribution of commercial agriculture work to nutrition but there is a need to accelerate the approach to strengthening food systems at country level, to help make sustainable and nutritious diets accessible to all. More generally, the department had begun to assemble learning on “what works” across nutrition-sensitive programming, but this is not yet fully embedded across the portfolio.
DFID’s evidence-based approach and effective programmes mean that the portfolio has strong potential to support reductions in undernutrition over the longer term. The Foreign, Commonwealth and Development Office (FCDO) and its partners will need to do more to strengthen nutrition work in sectors such as agriculture, and to develop a comprehensive intervention package that converges on the most vulnerable communities. ICAI has therefore awarded a green-amber score for DFID’s nutrition impact.
Recommendations
Although this report looks back at the work of DFID, our recommendations are directed to the FCDO following the merger of DFID with the Foreign and Commonwealth Office. They are intended to strengthen the new department’s future approach to nutrition.
Recommendation 1
FCDO should capture and communicate progress against all goals in its nutrition strategy, including strengthening systems and leadership for improved nutrition.
Recommendation 2
FCDO should strengthen statistical capacity and quality assurance in-country and centrally, to support more accurate measurement of programme coverage and convergence, and to use the data to improve nutrition programming.
Recommendation 3
FCDO should strengthen systems for identifying and reaching the most marginalised women and children within its target groups.
Recommendation 4
FCDO should more consistently gather citizen feedback to help improve and tailor its nutrition programmes.
Recommendation 5
FCDO should scale up its work on making sustainable and nutritious diets accessible to all, to help address the double burden of malnutrition, through nutrition-sensitive agriculture and private sector development.
Recommendation 6
FCDO should work more closely with its partners to achieve the convergence of nutrition interventions, by aligning different sector programmes to focus on those communities most vulnerable to malnutrition.
Introduction
“The livelihoods of many people became very hard, living like chickens not knowing what to eat the following day…”
“A lot of people were dying. Children and adults alike … my own children nearly died.”
Focus group participants, Shangombo District, Zambia
Malnutrition is a critical contributor to ill health, vulnerability, poverty and mortality. Worldwide, 820 million people are ‘chronically undernourished’ – 8.9% of the world’s population is believed to be hungry. Infants, young children and pregnant and breastfeeding women are most vulnerable to undernutrition. Their bodies have a greater need for nutrients per kilogram of body weight, such as vitamins and minerals, and are often more susceptible to the harmful consequences of deficiencies. 47 million children under five years of age are wasted, 14.3 million are severely wasted and 144 million are stunted. Undernutrition in children often leads to deficiencies in height and can impact brain development, meaning that full cognitive potential is not reached. Poor nutritional status in women often perpetuates a cycle of poverty and ill health for both the mother and her child. Children are at the highest risk of dying from wasting. Many infant and young child deaths in lower-middle-income countries are attributable to the poor nutritional status of the mothers. Malnutrition also encompasses overnutrition (the ‘double burden’) – a further 2 billion people are overweight or obese worldwide, according to UN joint estimates. The UK aid nutrition strategy is focused on tackling undernutrition, although it aims to minimise the risk of obesity.
Unsurprisingly, those countries with the highest burden of undernutrition are low- and middle-income countries. More than half of all stunted children live in Asia and more than one third in Africa. More than two thirds of wasted children under five live in Asia and more than one quarter in Africa. Across 53 countries, 113 million people experience acute hunger and 135 million people experience acute food insecurity as a result of conflict, climate shocks and economic turbulence, alongside structural factors related to poverty. Those already experiencing protracted crises, including in fragile and conflict-affected states, are more vulnerable to malnutrition.
Nutrition interventions are consistently identified as one of the most cost-effective development actions, with significant economic returns. Every $1 invested in reducing stunting can yield $11 in return. The Lancet Series has identified the ten key clinical interventions that can help solve the problem (see Box 4). However, reaching the most vulnerable with basic health care is complex in countries with few resources. Furthermore, UNICEF’s framework for the determinants of child undernutrition demonstrates that the problem has multifaceted causes and requires multifaceted solutions (see Figure 1). Undernutrition is a consequence of an inadequate diet and disease, such as diarrhoea, pneumonia and tuberculosis. These immediate causes are a consequence of limited access to sufficient and nutritious food, inappropriate maternal and childcare practices, inadequate health services and insanitary environments. Food, health and care are affected by social, economic and political factors including poverty, gender inequality, child marriage, poor education (especially for girls), political and economic marginalisation, and poor governance. These underlying factors explain why progress on reducing undernutrition is stalling in the poorest countries, and especially in the regions with the most vulnerable people within these countries.
Figure 1: Conceptual framework of the determinants of child undernutrition
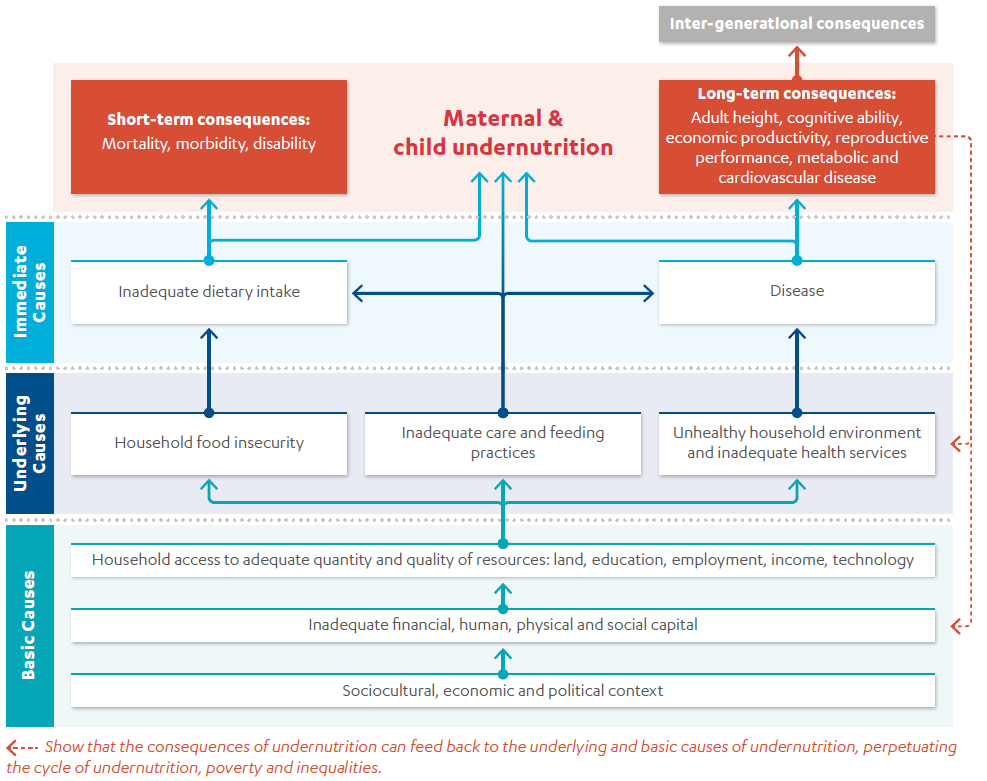
Source: Adapted from Improving Child Nutrition: The achievable imperative for global progress, UNICEF, 2013, p. 4.
Combatting malnutrition is both a development and a humanitarian priority worldwide. In 2012, the World Health Assembly endorsed the first ever global nutrition targets, which included tackling stunting, wasting, anaemia and low birth weight. At the Second International Conference on Nutrition in 2014, more than 170 governments committed to establish national policies and plans aimed at achieving the global nutrition targets. In 2015, world leaders enshrined these commitments in Sustainable Development Goal 2 and committed to end all forms of malnutrition by 2030.
However, most countries are lagging behind their targets and World Bank analysis highlights that there is still a large gap in the investment needed to reach the global nutrition goals. Data from UNICEF and the World Health Organisation shows that the number of stunted children under five in Africa increased from 50.3 million to 58.8 million between 2000 and 2018. Climate-related shocks and conflict are important drivers of this increase, with problems concentrated in the poorest countries and increasingly the poorest regions within countries. The global food system adds to the challenges of reducing malnutrition. Food chains prioritise processed products, to increase quantity of sales and profit margins, rather than nutritional quality, therefore making it difficult for consumers – especially those below the poverty line – to make healthy and affordable food choices.
Following the Nutrition for Growth Summit hosted in London, in 2015 DFID pledged to reach 50 million people. In late 2017, DFID launched its new global nutrition strategy to tackle undernutrition, prioritising support to the first 1,000-day window from conception through to two years of age, as well as preventing “the most severe forms of undernutrition” in children up to the age of five.
The coronavirus (COVID-19) pandemic is exacerbating the immediate and underlying causes of malnutrition and significantly threatens the potential for the global nutrition targets to be achieved. The World Food Programme has warned that an additional 130 million people could be pushed to the brink of starvation by the end of 2020. Due to preventative measures restricting the movement of people and goods, COVID-19 presents an unprecedented threat to economies, food systems and health systems. This could lead to an additional 1.2 million child deaths. The most vulnerable population groups, and those already experiencing protracted climate and conflict related crises, are likely to be disproportionately affected. The need for multi-sectoral action to combat the added pressures of COVID-19 and continue to deliver life-saving assistance is recognised by the global community. The coronavirus pandemic makes the topic of this review more relevant than ever.
This ICAI review assesses the accuracy of DFID’s claimed results (2015-19) and the robustness of the methodology used to calculate these results. It assesses the extent to which the nutrition portfolio targets and reaches the most vulnerable and hard-to-reach households, and the mechanisms used to understand their needs. Finally, the review assesses the impact of the nutrition programming that contributes to the reported results. This includes advocacy and technical assistance work at global and national levels, to foster action on nutrition.
The review questions were developed in 2019 to evaluate the UK’s current and previous work on nutrition, which at the time was being delivered through DFID. In order to maintain consistency with our approach paper, we have not updated these questions to reflect the merger of DFID into FCDO. As nutrition programming will continue, the questions remain relevant for continued UK programming.
Table 1: Review questions
| Review criteria and question | Sub-questions |
|---|---|
| Effectiveness: How valid are DFID’s reported nutrition results? | • How relevant is DFID’s results methodology? • How accurate are DFID’s nutrition results? • To what extent are DFID’s nutrition interventions achieving their immediate objectives? • What are the key factors influencing the achievement of immediate objectives? |
| Equity: Are DFID interventions reaching the most vulnerable and hard-to-reach women and children? | How well do DFID interventions reach the most vulnerable and hard-to-reach women and children? |
| Impact: To what extent is DFID helping to reduce malnutrition? | • Is DFID’s portfolio likely to achieve outcomes of reducing undernutrition over the longer term? • To what extent is DFID delivering high-impact interventions? |
Box 1: How this report relates to the Sustainable Development Goals
The Sustainable Development Goals (SDGs), otherwise known as the Global Goals, are a universal call to action to end poverty, protect the planet and ensure that all people enjoy peace and prosperity. Nutrition is relevant to several SDGs, most directly Zero Hunger (SDG 2) and Good Health and Well-being (SDG 3).
Related to this review:
![]() Goal 1: End poverty in all its forms everywhere. Preventing malnutrition is one of the UK’s primary objectives to tackle extreme poverty. Combatting malnutrition helps people escape extreme poverty, increases economic growth, and supports people to be more resilient in the longer term.
Goal 1: End poverty in all its forms everywhere. Preventing malnutrition is one of the UK’s primary objectives to tackle extreme poverty. Combatting malnutrition helps people escape extreme poverty, increases economic growth, and supports people to be more resilient in the longer term.
![]() Goal 2: End hunger, achieve food security and improved nutrition and promote sustainable agriculture. UK aid’s nutrition portfolio aims to combat malnutrition in women of childbearing age, adolescent girls and children under five. It aims to provide nutrition-specific and nutrition-sensitive services together to help maximise impact on malnutrition.
Goal 2: End hunger, achieve food security and improved nutrition and promote sustainable agriculture. UK aid’s nutrition portfolio aims to combat malnutrition in women of childbearing age, adolescent girls and children under five. It aims to provide nutrition-specific and nutrition-sensitive services together to help maximise impact on malnutrition.
![]() Goal 3: Ensure healthy lives and promote well-being for all at all ages. The nutrition portfolio aims to integrate nutrition services into wider health systems, strengthening those systems where possible through capacity building and technical assistance.
Goal 3: Ensure healthy lives and promote well-being for all at all ages. The nutrition portfolio aims to integrate nutrition services into wider health systems, strengthening those systems where possible through capacity building and technical assistance.
![]() Goal 6: Ensure availability and sustainable management of water and sanitation for all. DFID aimed to enhance the nutrition-sensitivity of its investments, including water, sanitation and hygiene. Clean water and sanitation can positively contribute to improved nutritional status, especially in children under five.
Goal 6: Ensure availability and sustainable management of water and sanitation for all. DFID aimed to enhance the nutrition-sensitivity of its investments, including water, sanitation and hygiene. Clean water and sanitation can positively contribute to improved nutritional status, especially in children under five.
![]() Goal 10: Reduce inequality within and among countries. UK aid’s nutrition portfolio demonstrates a commitment to ‘leaving no one behind’ through reaching the extreme poor and the most vulnerable. DFID’s establishment of nutrition target groups (women of childbearing age, adolescent girls and children under five) helps to tackle inequalities because undernutrition disproportionately affects these sub-groups.
Goal 10: Reduce inequality within and among countries. UK aid’s nutrition portfolio demonstrates a commitment to ‘leaving no one behind’ through reaching the extreme poor and the most vulnerable. DFID’s establishment of nutrition target groups (women of childbearing age, adolescent girls and children under five) helps to tackle inequalities because undernutrition disproportionately affects these sub-groups.
Methodology
To assess DFID’s nutrition approach and results at portfolio level and at programme level, this review adopted a methodology consisting of three components.
Figure 2: Methodological approach
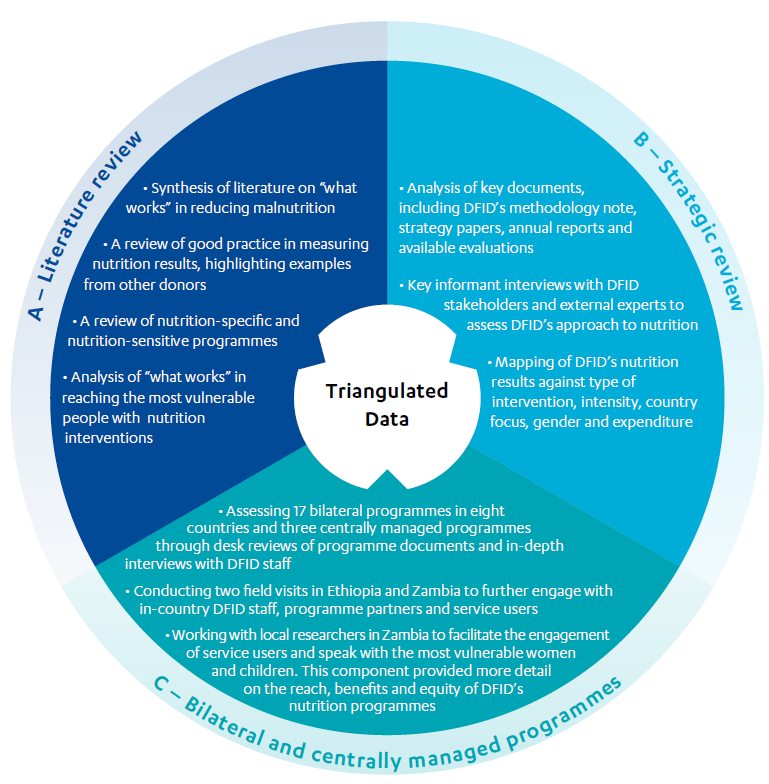
Component A – Literature review
A literature review was produced to identify areas of consensus around “what works” in reducing undernutrition.
Component B – Strategic review
Based on interviews with DFID staff and external experts, and desk reviews of key documents, including DFID strategies, annual reports, guidance documents and policies, we conducted a detailed assessment of DFID’s nutrition portfolio including its approach to calculate nutrition results. We also mapped DFID programme expenditure and results since 2015 against the intervention typologies including intensity of provision, the range of nutrition-specific and nutrition-sensitive interventions, country focus and gender split, as well as against stated targets in business cases and logframes. We also assessed the influencing role played by DFID within key international forums and partnerships to support the assessment of the department’s wider and longer-term impacts.
Component C – Bilateral and centrally managed programme assessments
Through a sample of 17 bilateral programmes implemented across eight countries and three centrally managed programmes, we have tested the quality of programme data that fed into DFID’s global results claims (see Annex 1 for a complete list of programmes and countries included in the sample). We also assessed DFID’s ability to reach the most vulnerable population groups through these programmes, and how far the programmes have aligned with best practice to reduce undernutrition, and triangulated these findings with evidence of impact. The programme reviews involved desk reviews of programme documentation (business cases, monitoring data, annual reviews and independent evaluations), followed by in-depth interviews with DFID programme managers. A detailed assessment framework was used to gather, analyse and triangulate evidence for each programme, enabling systematic analysis against each review question.
We also conducted analyses at country portfolio level, across eight countries. This was to help assess whether DFID had adequately mitigated the risk of double-counting results, and to understand the extent of multi-sector programming and integration of activity, as well as broader impacts on undernutrition. In two of these countries, Ethiopia and Zambia, we conducted field visits, which enabled us to engage in more depth with programme partners, external stakeholders and service users, and explore whether programmes are reaching the most vulnerable, as well as strengthening government systems and capacity.
In Zambia, we undertook a longer visit to enable more in-depth engagement with service users and citizens. We worked with national researchers to identify and access vulnerable women and children involved in DFID’s programmes. Semi-structured interviews and focus group discussions were undertaken in hard-to-reach programme areas, supported by clear guidelines and ethical protocols. This helped ensure that the voices of ordinary citizens were reflected in our findings and recommendations.
Box 2: Limitations of the methodology
Review scope and coverage: The multi-sector nature of nutrition programming, as well as the range of intensities and fragile/non-fragile state locations, presented a challenge for the review as a very large potential scope of work. We therefore narrowed the scope of the review to ensure sufficient depth. Work focusing on the macro-level drivers of nutrition outcomes, such as climate change, trade, economic growth, food prices and land use policies, is not included within the scope of the review. The review’s focus is on DFID’s achieved results and impact, although the evolving strategic approach is considered.
Data on effectiveness and equity: The nutrition portfolio’s results data are aggregated from individual programmes but come from a variety of secondary sources. We were not able to complete detailed verification exercises with the data. Instead, we interrogated the indicators, methodologies and assumptions behind the data, and triangulated reported results with other sources. For example, to help understand whether the most marginalised have benefited from DFID’s nutrition programming, we included a programme of service user consultation. However, this only represents a small sample of citizens.
Data on impact: The long causal pathways associated with reducing undernutrition (and associated measures of stunting and wasting), the range of other actors involved and frequent data limitations means that assessing and attributing impact at country level is challenging. To provide a credible assessment of impact, we triangulated a range of available evidence. This included the extent to which DFID’s nutrition strategy and interventions have been aligned with global literature on “what works”, evidence of shorter-term programme effectiveness (in other words nutrition outcomes, such as dietary improvements or changes in feeding practices), and evidence of programme impact from robust external evaluations.
Background
The UK government is a leading advocate for tackling malnutrition in the world’s poorest countries. Following the UK’s hosting of the global Hunger Summit during the London 2012 Olympic Games, in 2013 the UK co-hosted the first Nutrition for Growth Summit. This aimed to galvanise global efforts to tackle undernutrition, helping to secure £2.7 billion in new financial commitments from donors, alongside £12.5 billion from nutrition sensitive investments. DFID’s subsequent pledge in 2015 to reach 50 million people was a significant advance on the UK’s previous goal of reaching 20 million people from 2011-15. In 2015, DFID disbursed a record $1 billion of official development assistance to nutrition-specific and nutrition-sensitive programmes, reportedly reaching a total of 13.3 million children under five, women of childbearing age and adolescent girls. The share of bilateral aid spent on nutrition grew from 9% in 2013 to 11% in 2017, reflecting global increases in spend on nutrition. Box 3 provides a summary of DFID’s nutrition approach and goals.
Box 3: DFID’s nutrition approach and goals
Following the UK’s commitment in 2015 to reach 50 million people through nutrition services, DFID’s Global Nutrition Position Paper (2017) set out new priorities for scaling up nutrition interventions:
- preventing wasting, micronutrient deficiencies and low birth-weight, alongside existing work to prevent child stunting
- addressing the nutritional needs of women and adolescents, particularly adolescent girls
- strengthening the breadth and quality of DFID’s nutrition-sensitive multi-sector investments
- enabling countries to be ready for the future by strengthening leadership and delivery, and by building resilience to future shocks
- achieving a global architecture for nutrition that works in support of countries that face a high burden of malnutrition
- improving the quality and availability of nutrition data.
In addition, DFID also outlined the following objectives:
- Increasing its support for nutrition-sensitive interventions to address the underlying and root causes of malnutrition alongside nutrition-specific services in the same places, to maximise impact and improve value for money.
- ‘Leaving no one behind’ by focusing on reaching the extreme poor, the most marginalised and those in fragile and conflict affected states.
- Preparing for the future by supporting government leadership, capacity and system strengthening to deal with current and new challenges to nutrition, including from climate and environmental change and urbanisation.
- Leveraging private sector investments that are beneficial to nutrition – for example, by helping to remove barriers that prevent poor people from accessing markets for nutritious foods and promoting responsible business behaviour.
DFID also committed to empower international leadership and coordination, facilitate effective action by multiple partners and actors, drive innovation and build evidence of good practice, and promote accountability on a global scale by leading by example.
DFID’s approach to nutrition programming has reflected the global literature by classifying interventions into two groups: ‘nutrition-specific’ and ‘nutrition-sensitive’. Nutrition-specific interventions aim to address the problem directly (and include nutrient supplementation for women and children, support for infant and young child feeding, and treatment of acute malnutrition). Nutrition-sensitive interventions are those that address the multiple underlying causes of undernutrition (for example a lack of access to safe water and sanitation – which leads to diarrhoeal disease, food insecurity and inadequate health care systems). While the evidence base is strongest for nutrition-specific programmes (see Box 4), both are needed to tackle undernutrition sustainably.
Box 4: The nutrition-specific intervention package with a strong evidence base
A 2013 Lancet article identified the ten nutrition-specific interventions with the strongest evidence for contributions to reductions in child mortality. These are:
- periconceptional folic acid supplementation or fortification
- maternal balanced energy protein supplementation
- maternal calcium supplementation
- multiple micronutrient supplementation in pregnancy
- promotion of breastfeeding
- appropriate complementary feeding
- vitamin A supplementation in children aged between 6 and 59 months
- preventive zinc supplementation in children aged between 6 and 59 months
- management of severe acute malnutrition
- management of moderate acute malnutrition.
If these ten interventions were to be scaled up to 90% coverage, the authors argue that the current total of deaths in children younger than five years can be reduced by 15%, stunting reduced by 20.3% (33.5 million fewer stunted children) and the prevalence of severe wasting reduced by 60%.
UK aid’s portfolio of nutrition programmes therefore span a range of sectors. In some countries, DFID has supported stand-alone, multi-sector nutrition programmes, which integrate nutrition-specific interventions with WASH (water, sanitation and hygiene), nutrition-sensitive agriculture and livelihoods, women’s empowerment, and/or education campaigns. In other countries, DFID has mainstreamed nutrition across different sector programmes, such as humanitarian response, social protection and private sector development. According to a classification of DFID’s nutrition projects, 40 out of 147 in 2017 included both nutrition-specific and nutrition-sensitive components.
DFID’s methodology to calculate its nutrition results and reach has also evolved. Up to 2015-16, DFID defined ‘reach’ as “the number of children under five, and breastfeeding and pregnant women reached through DFID’s relevant projects”. However, this did not distinguish between those people reached by a single nutrition intervention, and those receiving both nutrition-specific support and nutrition-sensitive interventions tackling underlying causes. Since 2015-16, DFID classified reach into high, medium and low intensity, with the aim of promoting a ‘convergence’ of interventions on target groups (see Figure 3).
Figure 3: DFID’s intensity classification of nutrition interventions
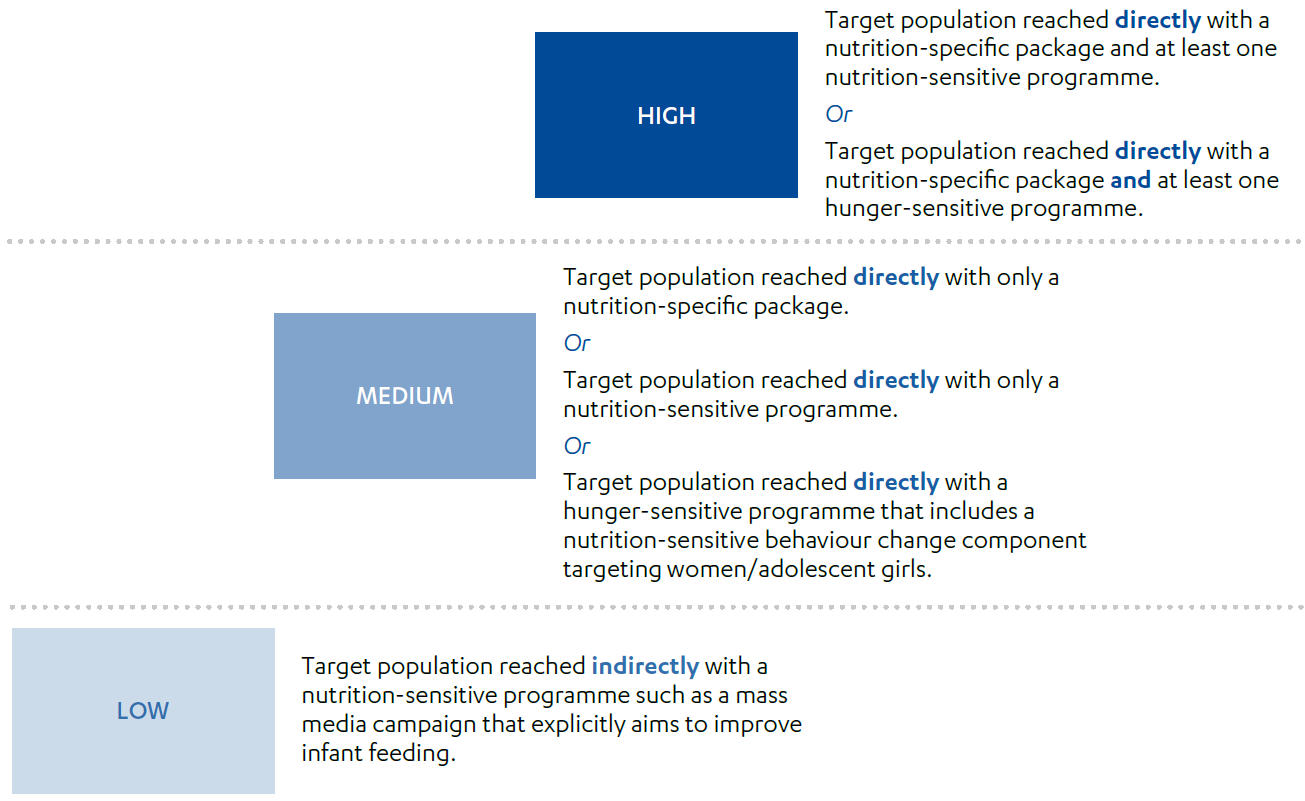
DFID’s methodology note introduced further criteria to encourage the reporting of quality results. Results should only be counted as nutrition-specific if a woman or child is receiving a comprehensive package of support, and if the treatment for acute malnutrition is successful. Nutrition-sensitive results should only be counted where a programme has a clear nutrition objective and outcomes and impacts are being monitored, and ideally where there is evidence of nutritional change.
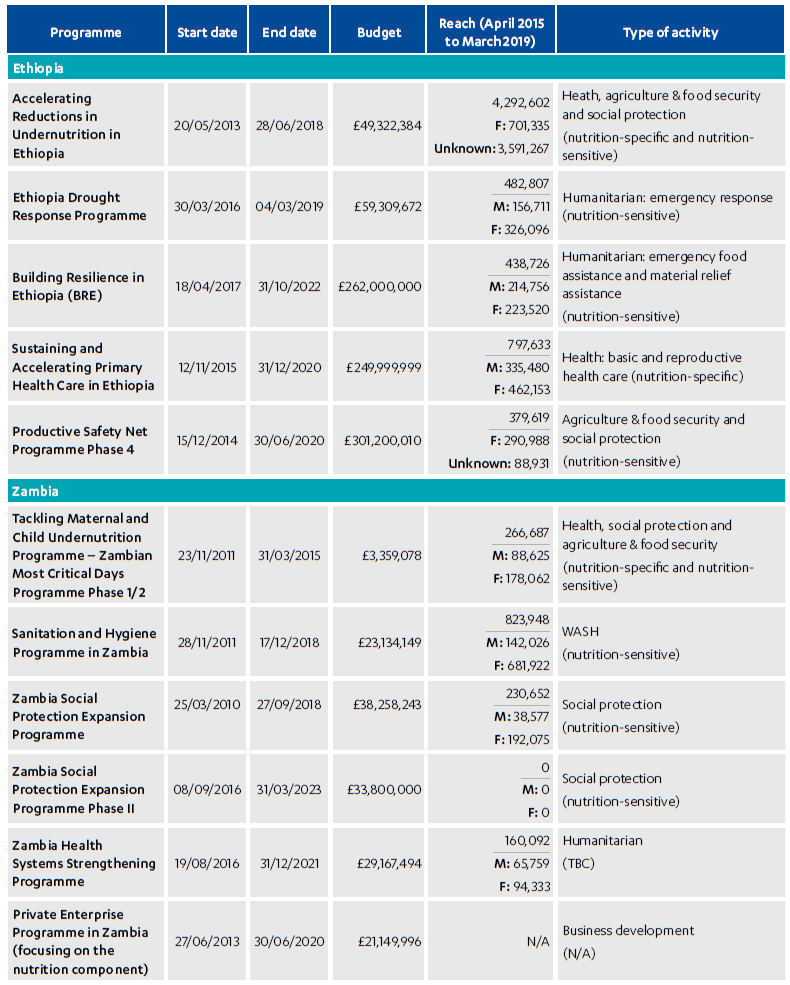
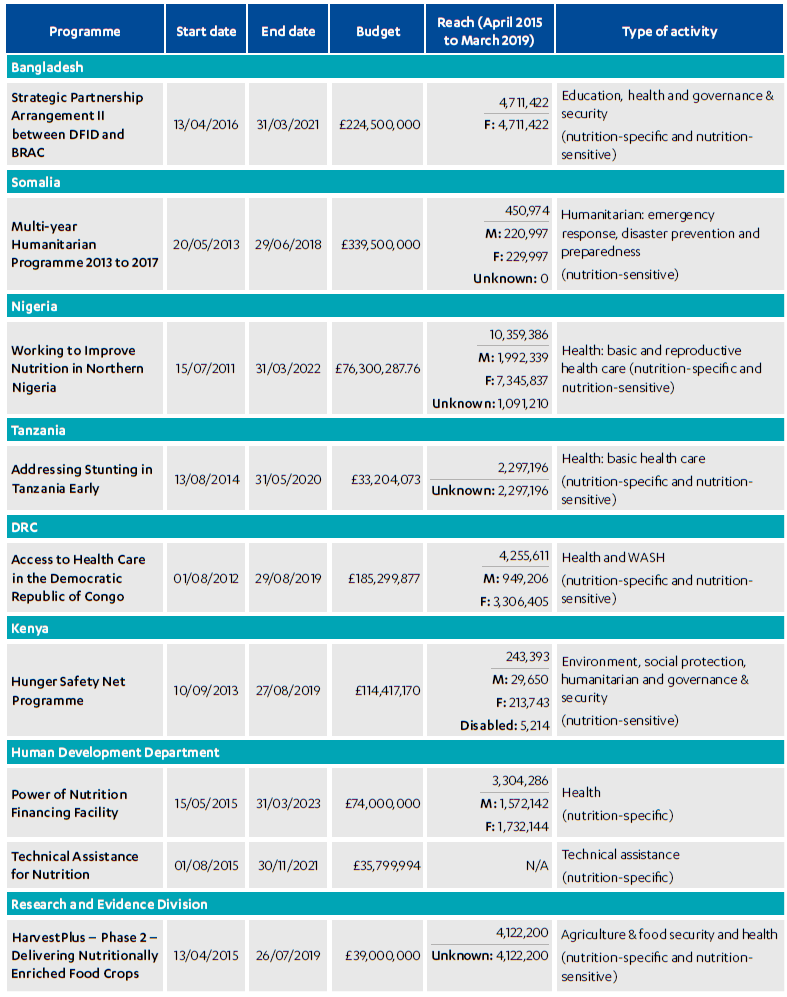
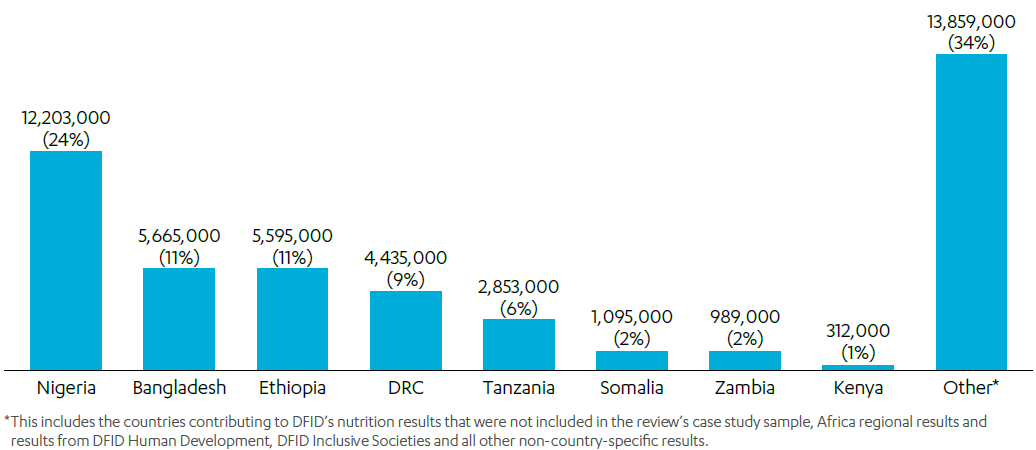
The nutrition portfolio’s results from bilateral programmes span 23 countries across Africa, South Asia, the Middle East and South East Asia (the remainder come from centrally managed and other non-country-specific programmes). The eight countries covered by this review account for 65% of DFID’s nutrition results or reach overall, between 2015 and 2019 (see Figure 4).
Figure 4: Number of children under five, women of childbearing age, and adolescent girls reached in review countries and their contribution to DFID’s nutrition results (%) (2015-2019)
In addition to reaching the most vulnerable, a further priority for the nutrition portfolio is eradicating undernutrition over the longer term. DFID recognised that it could not do this alone and should work with and help strengthen the capacities of other actors, not least governments, to achieve adequate coverage of services and sustainable impact. The 2017 Nutrition Position Paper frames DFID’s advocacy and technical assistance work as central to this goal. Through this work, DFID aimed to build the necessary leadership, capacity, funding and action to tackle undernutrition, working with global and national partners. Programming includes the centrally managed Technical Assistance for Nutrition programme (£35.8 million), through which UK aid supports the Scaling Up Nutrition (SUN) Movement and strategy development within SUN countries.
In 2014, ICAI reviewed DFID’s emerging work on nutrition, awarding it a green-amber score. While there were promising signs of progress, ICAI found that the potential impact of the portfolio could be increased through more targeted and integrated interventions (see Box 5). At the time of the review, however, it was too early to tell whether DFID’s nutrition programmes had been successful, with very few evaluations completed. With this current review, we have had more evidence from which to assess effectiveness and impact, as well as for checking DFID’s results. Now is a timely opportunity to provide an update on progress.
Box 5: Key findings and recommendations from ICAI’s 2014 nutrition review
Findings:
- DFID played a key role in mobilising the global community to invest in nutrition through the scale-up of its own work since 2010.
- The pace and scale of DFID’s global work was positive, although country-level programme implementation could have been more rapid.
- DFID’s work was appropriately balanced between nutrition-sensitive and nutrition-specific programming and was based on sound evidence. However, nutrition-specific and nutrition-sensitive programmes were not always implemented in the same communities, and the nutrition-specific package was not always focused on interventions with the greatest impact on stunting.
- DFID provided valuable technical assistance to build government delivery capacity and was effectively coordinating with other donors.
- Service users were appropriately involved in the design of projects, but projects needed to be tailored to target the most vulnerable and hard-to-reach children better.
- DFID’s use of reach figures had limitations as they only measured a single intervention and was often based on unverified assumptions.
- Theories of change required a greater focus on intermediate outcomes and risks, and DFID needed to improve the monitoring of its programmes and ensure that results were not over-reported.
Recommendations:
- DFID should make longer-term commitments to maintain the pace and scale of its nutrition investments.
- DFID should target the most vulnerable and hard-to-reach mothers and children better.
- DFID should invest in country- and global-level systems that generate robust data on nutrition.
- DFID should explore how to effectively engage the private sector to reduce undernutrition.
Findings
In this section, we set out our findings on the accuracy of DFID’s claimed nutrition results (2015-19) and the effectiveness of the nutrition programmes in achieving their immediate goals. We also include our findings on DFID’s ability to reach the most vulnerable citizens, and the likely longer-term impact of the department’s strategy and programmes on undernutrition, based upon the available evidence.
Effectiveness: How valid are DFID’s reported nutrition results?
The measurement of reach is innovative and drives an increased focus on quality programming, although it does not reflect all goals within UK aid’s nutrition strategy
DFID’s nutrition results are based on the number of children under five, women of childbearing age and adolescent girls reached by nutrition programmes. Responding to a key criticism of the 2014 ICAI review (see Box 5, above), as well as the general limitations of a results measure based on reach, in 2015-16 DFID introduced the intensity classification. The intensity classification closely reflects the scientific evidence on what works: that combined nutrition interventions (high-intensity reach) will have a greater impact on nutrition than nutrition-specific or nutrition-sensitive programmes alone (medium- and low-intensity reach). By counting individuals who receive multiple interventions, and including other quality criteria (see para 3.5), the new methodology has driven the reporting of more meaningful nutrition results.
ICAI found that reporting against the global target of reaching 50 million people with nutrition services has been helpful for increasing a general focus on nutrition within DFID, and prioritising this within country offices. Country staff told ICAI that the revised results methodology has also helped them to scrutinise the effectiveness of their nutrition programmes more closely, and to hold key delivery partners (such as UNICEF) to account. Specifically, counting high-intensity reach has encouraged country advisers to think about how to achieve the convergence of different nutrition programmes to achieve greater impact for vulnerable populations. This also responds well to a key finding from the 2014 ICAI review, that DFID needed to make greater efforts to implement different programmes in the same communities.
DFID used the guidance to count broadly relevant nutrition-specific and nutrition-sensitive activities in the portfolio’s reach results. Nutrition-specific interventions relate to the high-impact package recommended by The Lancet, including the provision of vitamin A supplements, deworming tablets, iron and folic acid tablets, and counselling on infant and young child feeding. Nutrition-sensitive results come from a range of relevant interventions, from water, sanitation and hygiene (WASH), women’s empowerment and small-scale agriculture through to social protection. Some programmes, including in Ethiopia, Tanzania and Zambia, span both (see Box 6).
Box 6: Tackling Maternal and Child Undernutrition Programme, Zambia
The Tackling Maternal and Child Undernutrition Pilot Programme (2011-13) aimed to improve nutrition by delivering vitamin A and deworming tablets to children in nine districts of Zambia and was assessed by ICAI in its 2014 review. Phase I of the programme (2013-18), known as Zambia’s First 1,000 Most Critical Days Programme (MCDP), was launched through a pooled Scaling Up Nutrition (SUN) fund with contributions from DFID, Swedish International Development Cooperation Agency (SIDA) and Irish Aid.
MCDP is a multi-sector programme that aims to reduce stunting in Zambia to 25% in targeted districts by focusing on the most critical period: the first 1,000 days of a child’s lifetime. The programme focuses on scaling up a set of routine evidence-based nutrition-specific interventions proven to reduce stunting. As the theory of change highlights, improved nutritional intake is necessary but not sufficient to improve nutrition outcomes. Therefore, nutrition-sensitive interventions, for example promotion of safe water, hygiene and sanitation and complementary feeding, are implemented alongside these direct nutrition-specific interventions. Volunteers from different sectors often come together to conduct joint community outreach activities. Because the programme aims to ‘converge’ the package of services on the same population, programme results are classified as high-intensity.
Through focus groups with local citizens, ICAI heard how they have had access to infant and young child feeding counselling, seeds (beans, groundnuts and sorghum), and treatment and care for acutely malnourished children. Households are taught to grow, preserve and consume a diverse range of more nutritious foods. Service users highlighted their increased knowledge of good nutritional practice:
“A child should be given different types of food. Vegetables, foods that give energy like nshima, fish and the body building foods, they are important for the health of a child and for the child’s growth.”
“We add groundnuts to the porridge, sugar or milk.”
Focus group participants, Sioma District, Zambia
Under Phase I of MCDP, DFID reported that it reached 266,687 women of childbearing age and children under five during its ‘peak year’. This is a pro-rated estimate based upon DFID’s financial contribution to the pooled fund. An independent evaluation found positive effects on feeding practices, young children’s nutritional intake and reduced probability of diarrhoea, relative to children in comparison districts, as well as reductions in stunting among target districts for children aged between six and 23 months. However, less progress was made on increasing the coverage and take-up of nutrition-specific services (iron and folic acid supplements and deworming pills) by pregnant women, and effective convergence of services was not always possible to achieve in practice, due to the difficulty of coordinating different government sector budgets.
The programme has also helped increase engagement from senior leadership within the Zambian government and the political prioritisation of nutrition. For example, in 2018 Zambia hosted a National Nutrition Summit, supported by DFID, UNICEF and other partners, where the vice president announced several commitments, including allocating budgets to prevent stunting. Phase II of the programme (2019-2021) supports the scale-up of interventions to over 30 districts and is currently funded by the UK, the government of Zambia, the US, Germany and Sweden. In addition, USAID provides funding for a learning and evaluation component. The EU is also planning to support Phase II.
The results methodology does not capture wider strategic commitments and contributions to nutrition, achieved through advocacy and technical assistance work. These have included securing political commitment and systems strengthening, leveraging the private sector, and fostering effective international leadership and coordination. ICAI found that DFID has not systematically reported on these results. This represents a missed opportunity to communicate and learn from DFID’s overall ‘story of change’. By contrast, USAID reports on progress against all of the objectives within its Multi-Sectoral Nutrition Strategy (2014-2025), guided by a monitoring and learning plan. USAID undertakes three periodic assessments to monitor progress and gather evidence for learning (the first of which was undertaken in 2019).
DFID data shows that it met its global nutrition target (50 million people), despite taking a conservative approach to estimating its overall reach
DFID reported that 50.6 million women, children under 5 and adolescent girls were reached by its nutrition interventions over the period 2015-19. Figure 5 shows all countries which contribute to DFID’s overall nutrition results, by volume.
Figure 5: DFID’s nutrition results by country (number of children under five, women of childbearing age, and adolescent girls reached, 2015-19)
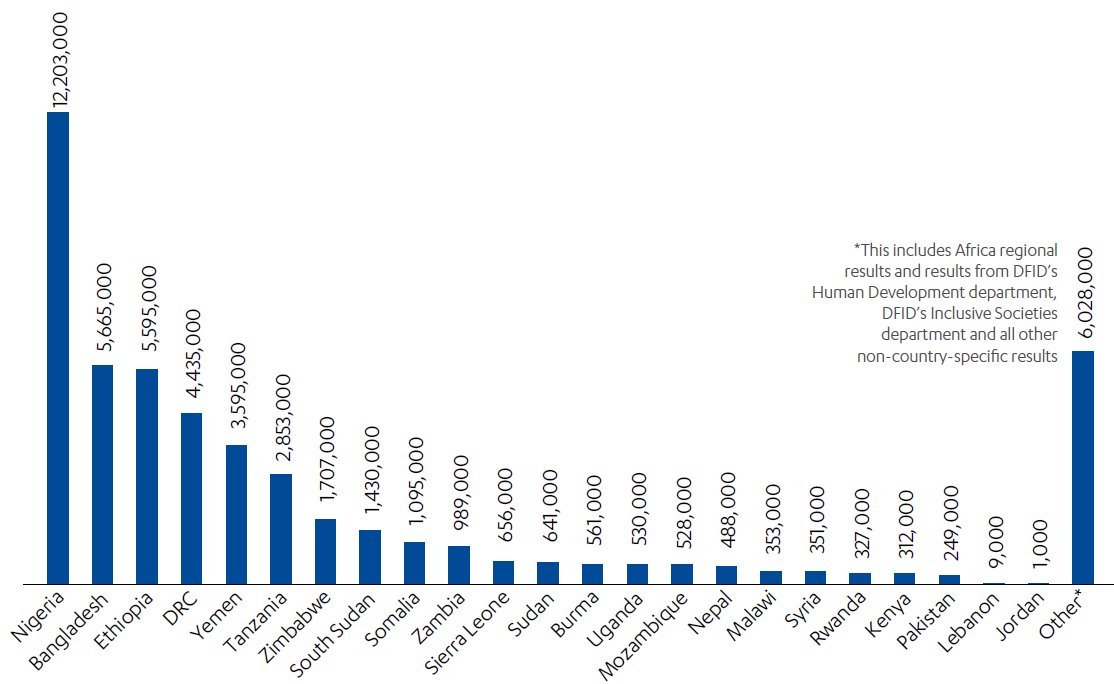
Source: DFID results dataset 2018 to 2019, DFID, 2019, link. The data for this graph has been taken from Table 8 of the dataset: Number of children under five, women of childbearing age and adolescent girls reached by DFID through nutrition-related interventions.
While ICAI found some inaccuracies for individual programmes (see paras 4.9 to 4.15), overall DFID has taken a cautious approach to estimating its global nutrition results, avoiding overstatement of its success. In the case of some programmes, DFID’s reported results are likely to represent an underestimation of true reach. On this basis, ICAI concludes that DFID’s nutrition result is broadly valid. DFID has taken a conservative approach to estimation through adopting the following methods:
- Avoiding double-counting the same individuals benefiting from different programmes, different components within the same programme, and nutrition support received over multiple years.
- Adjusting its programme results downwards where other donors are providing funding, based upon its proportional funding contributions.
- Excluding results from programmes which could potentially be classified as nutrition-sensitive, but which neither had a clear nutrition objective, nor were monitoring nutritional improvement, in line with the results guidance. The clearest examples of this relate to WASH programming.
In January 2020, a major revision resulted in DFID’s nutrition reach being revised downwards by 9.7 million people (from 60.3 million). DFID’s central nutrition team and country office staff had identified potential double-counting in Somalia and Yemen and within the Power of Nutrition programme. The revision also incorporated further improvements to the quality of the results data, including in the attribution of results to DFID (based upon the latest financial information), and the exclusion of children unsuccessfully treated for malnutrition (in Yemen). DFID provided a public amendment and statement explaining these changes.
There have been inaccuracies and inconsistencies in the results measurement for some nutrition programmes. The nutrition portfolio has faced challenges in classifying intensity
Generating an accurate picture of reach within a country is important, since increasing the population coverage of nutrition services is a critical element of the nutrition strategy and theory of change. As noted in the Lancet Series and DFID’s methodology note, population coverage of 90% is required for the nutrition-specific package to have a significant impact on stunting and wasting.
The nutrition portfolio’s results reporting is more sophisticated than before, but the downward revision of the global figure highlights the difficulties with the methodology. ICAI found that reporting against the nutrition results framework has been a complex and resource-intensive exercise for staff. Not all programmes were previously monitoring reach in the same way, and it has taken time to align and improve existing processes. Errors and inconsistencies have arisen in some instances. From the 12 programmes where we reviewed their accuracy in depth, ICAI found the results for one programme to be “very reliable”, seven “reliable” and four “less than reliable”. This assessment was based upon a review of the calculation methodologies employed (including whether actual or estimated results figures were used), and the approach to avoiding double-counting, as well as comparisons with other programme monitoring data and discussions with responsible officers.
Reliance on poor-quality programming and especially national data systems has been one of the most significant challenges for DFID in accurately calculating its nutrition reach (which is why the department has been working to improve systems in some countries). This weakness is recognised in the methodology note, and ICAI found several examples of this in practice. In some countries, a lack of robust monitoring data means that nutrition results are estimated based on local population data (in turn derived from national census data of variable quality). Results in Tanzania had to be revised several times – the country’s nutrition programme did not have a robust methodology in place for measuring the reach of a mass media educational campaign. It was concluded that the reported results were too conservative. One inaccuracy observed by ICAI related to a simple human error made in counting results.
Other problems related to inconsistency in the approaches to aggregating nutrition results across countries and avoiding double-counting. The country team in Ethiopia disaggregates programme results by region, and then adjusts the results based upon the estimated geographical overlap in each region. This is more sophisticated than approaches observed in some other country teams, which apply a more arbitrary percentage reduction at country level. ICAI found that country teams have developed their own data sheet for aggregating country results, which is contributing to inconsistency as well as duplication of effort. Errors and inconsistencies increase the requirement for quality assurance and the burden on the department’s statistical cadre.
Recognising these challenges, the statistical cadre and central nutrition team have provided an important quality assurance function at the global level to supplement the quality assurance conducted by programme teams as an ongoing part of programme monitoring. However, they have not always immediately spotted errors (for example in the case of the major revision noted above) for a range of reasons. Ensuring regular, scheduled quality assurance of the results is an important way to spot and address errors. ICAI also found that statistical capacity has not always been sufficient within country teams. Quantitative skills and capacity are required not only to help avoid double-counting, but also to provide longer-term support for strengthening monitoring and data systems to measure coverage more accurately. For example, DFID said that the Democratic Republic of Congo (DRC) office now has a new statistics officer who is helping to improve monitoring systems, calculate reach more accurately, and classify programme results by their correct intensity.
ICAI also found evidence that DFID has been underestimating its high-intensity reach. Most of the nutrition results (over 60%) are classified as medium-intensity. DFID improved in classifying the intensity of its results in 2019, with only 3.5% of results not classified (compared with 16.4% in 2018). However, country teams have faced challenges in identifying high-intensity reach. In most cases, this is because programme or country management information systems are not yet sophisticated enough to record whether individuals have received services from different ministries. Ethiopia has not reported high-intensity reach at all, despite its Accelerating Reductions in Undernutrition programme (with 4.3 million people reached) providing a package of interventions across a range of sectors. DFID Zambia, in collaboration with USAID and the Zambian government, planned to introduce at least two indicators to measure the convergence of services at the household and health facility levels through surveys.
The other main area of inconsistency across country teams has been in the treatment of nutrition-sensitive programmes. The country team in Zambia classifies its nutrition-sensitive programmes as low-intensity, due to their lack of a targeted approach. However, two of these programmes, covering social protection and WASH, also had no nutrition objectives or clear indicators at the outcome and impact levels. The impact on nutrition was, however, assessed by the evaluations for these programmes. By contrast, the Ethiopia country team decided not to include any low-intensity results, in part due to the risk of double-counting. In the case of WASH, Ethiopia’s programme was excluded noting that its impact on nutrition has not been measured and that the evidence for a direct impact of WASH on nutrition outcomes is mixed. ICAI found that DFID’s methodology note lacks sufficient detail on which activities can be considered nutrition-sensitive and on relevant indicators.
DFID’s methodology note also encourages country teams to provide brief narrative reports outlining what is being done to strengthen national policies, the coverage and effectiveness of nutrition interventions, and monitoring systems. However, ICAI found that these narratives and associated lessons learnt have not been systematically collected by country teams or shared internally or externally. As a result of this and data limitations, ICAI found that the portfolio’s nutrition results are not consistently used to improve programme implementation. For example, there is scope to link the learning from measuring high-intensity reach with planning for improving the convergence of programmes on vulnerable populations and improving national data systems. This could in turn be linked to performance indicators to measure and report better on the impact of UK aid on systems strengthening.
More than half of the nutrition programmes assessed by ICAI have achieved their immediate nutrition objectives
Since the 2014 ICAI review, DFID made significant progress in implementing its nutrition programmes, and overall they are judged to have been effective in delivering their immediate objectives.
Of the 20 nutrition programmes reviewed by ICAI (see Annex 1), more than half (13) have met most (at least three quarters) of their output targets. Five programmes met more than a quarter but less than three quarters of their output targets. Two programmes had not met any output targets relevant to nutrition.
- Eight programmes showed strong performance on delivering nutrition-specific outputs. These include the provision of vitamin A, iron and folic acid supplements, counselling on child feeding and maternal nutrition (and associated training for health workers), and the management of moderate and severe acute malnutrition. For example, between 2011 and 2017, the Working to Improve Nutrition in Northern Nigeria programme reached 10,086,704 children under five with vitamin A supplementation, 7,469,116 pregnant women with iron supplementation and 814,437 pregnant women and mothers of young children with feeding counselling.
- At least six programmes, including several in Ethiopia and Zambia, delivered strongly on outputs despite operating during humanitarian crises caused by droughts, floods and/or conflict. For example, between 2012 and 2016, over 200,000 children with severe acute malnutrition were treated at community sites in Northern Nigeria. Conversely, three programmes struggled in humanitarian contexts, due to challenges with partner coordination and government delivery capacity, as well as reaching the poorest regions. For the Productive Safety Net Programme 4 in Ethiopia, this resulted in delays in the distribution of food transfers.
- Six programmes demonstrated positive progress in engaging with government, and delivering outputs related to strengthening government leadership, coordination and delivery capacity. The Power of Nutrition centrally managed programme also contributed positively to supporting government engagement, although it did not meet its targets to leverage additional funds for nutrition from other donors, philanthropists, the private sector and high-net-worth individuals. DFID reported that the programme has since been working with the Bill and Melinda Gates Foundation to adjust its investment model and increase private sector and philanthropic contributions.
Progress on delivering nutrition outcomes is more mixed, although positive overall. 11 of the 16 programmes measuring outcomes relevant to nutrition have met most (at least three quarters) of their outcome targets. Two programmes have met some (more than a quarter but less than three quarters) of their outcome targets, and three programmes have met less than a quarter of their targets.
- Six programmes reported positive outcomes highly relevant to nutrition, including improved breastfeeding and complementary feeding knowledge and practices, an increase in dietary diversity and meal frequency among women and children, and reductions in severe acute malnutrition. Programmes that provided more comprehensive packages of nutrition-specific support tended to deliver more positive nutrition outcomes. Citizens living in Mongu District, Zambia explained:
“Way back we never used to know about feeding and what the baby requires. We didn’t know that we can eat goat milk or even put meat or pumpkin leaves in the porridge but because of this programme we have come to learn about it. We just used to give them soup and plain porridge but that’s no longer the case.”
Focus group participant, Mongu District, Zambia
- Four further programmes reported successfully increasing population access to nutrition services – including feeding counselling and vitamin A supplementation. Although these programmes assessed their impact on nutrition (through measures of stunting), they lacked any further outcome indicators beyond coverage (for example influencing feeding practices or diets). Without this, it is difficult to judge the quality of support received and their specific contribution towards reductions in undernutrition.
- Through advocacy and technical assistance, four country-based and one centrally managed programme (see Box 7) reported successfully strengthening the capacity of government systems for planning, coordinating and delivering nutrition services. For example, and despite initial delays in procuring technical assistance, Building Resilience in Ethiopia reported progress in supporting the government to lead and manage humanitarian response services better. This includes building early warning systems (‘hot spot mapping’) that can anticipate local droughts and crop failure, support early intervention and help avert larger nutrition crises.
Box 7: Achievements of the Technical Assistance for Nutrition programme
The Technical Assistance for Nutrition programme funds technical assistance and knowledge management for the Scaling Up Nutrition (SUN) Movement through Nutrition International, Maximising the Quality of Scaling Up Nutrition Plus (MQSUN+) and the Emergency Nutrition Network, as well as providing direct support for the SUN Movement Secretariat. The programme has also provided technical assistance capacity to country teams. Overall, the programme has helped to strengthen governance, capacity and knowledge management for nutrition at global and country levels. Key contributions have included ensuring that evidence-based, costed country action plans are in place, for example in Somalia, Afghanistan and Ethiopia, and developing national nutrition policies and programmes for Madagascar, Kenya and Uganda, behind which donor investments can then align. In Ethiopia, the implementation of the Seqota Declaration, a multi-sector plan to eradicate the underlying causes of chronic undernutrition and end child stunting by 2030, has been supported by the programme. Technical Assistance for Nutrition has also helped develop budget tracking and other systems to review progress. Globally, the programme has effectively built the capacity of country teams to deliver on their nutrition and humanitarian goals, through the MQSUN+ mechanism and the production of various knowledge outputs and guidance (including in areas relating to equity). Its success has been aided by its flexible and demand-driven approach, and range of expert and nimble partners able to operate in this way, as well as proactive engagement from staff.
Based upon evidence of outputs and outcomes, the nutrition-sensitive components of some multi-sector programmes have sometimes been less effective. The small number of nutrition programmes with integrated WASH components have had less success in delivering behaviour change in hand washing and using clean sources of drinking water. The Productive Safety Net Programme in Ethiopia, a social protection programme that integrates nutrition-sensitive behaviour change activities and small-scale food production (alongside its general aims of reducing poverty), has faced challenges including the low uptake of nutrition counselling (which involves providing advice on feeding and hygiene practices). This suggests that a more intensive approach might be needed for these activities, either within multi-sector nutrition programmes or through convergence with other programmes.
Three programmes have not met any outcome targets relevant to nutrition. The Hunger Safety Net Programme in Kenya provides an example of some of the typical challenges faced.
Box 8: Challenges faced by the Kenya Hunger Safety Net Programme
The Hunger Safety Net Programme (2013-19) in Kenya was classified as a low-intensity, nutrition-sensitive social protection programme. While it broadly fulfilled its function as a safety net for the extreme poor, DFID reported that the programme fell slightly short of its outcome targets, including for the quantity and quality of food consumption. This reflects failures in delivering cash payments to some users, linked to weak financial infrastructure within target districts and late government payments. While the programme successfully developed a model social safety net for Kenya, scalable to support early crisis response, and DFID influenced the government’s social protection policy, systems were not strengthened to the extent required to ensure full coverage and sustainability. This is attributed to overambitious targets and external factors beyond the programme’s control (including Kenya’s existing budget deficit). DFID responded by increasing the flexibility of its own financial contributions and extending the programme into a third and final phase.
For four programmes, outcomes relating to undernutrition or its underlying causes were not being monitored sufficiently. Logframes for some nutrition-sensitive programmes, including in private sector development and social protection, lacked the most relevant outcome indicators. One WASH programme was focused on monitoring outputs rather than outcomes. Two programmes were not monitoring nutrition outcomes despite having relevant nutrition indicators in their logframes. This was due to a lack of relevant data collection methods and targets. DFID said that improvements were planned.
Where relevant nutrition outcomes are being monitored, ICAI finds that the nutrition portfolio has often collected high-quality and globally recognised performance data, such as indicators of dietary diversity and minimum acceptable diets, working with implementing partners such as UNICEF. However, overall, ICAI found room for improvement in the monitoring of outcomes among those programmes contributing to nutrition results. This was particularly the case for nutrition-sensitive programmes. Because of this, it is not always straightforward to judge their effectiveness (and “what works”), and some programmes needed a sharper focus on nutrition. Now a more comprehensive results framework is being developed, linked to an overarching ‘nutrition theory of change’. Examples of relevant intermediate outcomes and impacts are also included within DFID’s recently finalised value for money guidance. Programmes need to draw on this to help improve the consistency of their outcome measurement, including underlying causes.
Factors commonly influencing the effectiveness of the nutrition programmes include effective political leadership and coordination mechanisms, national and community-level delivery capacity, and systems for data and learning. External shocks are a major constraint
We identified a range of enabling factors that influence the effectiveness of nutrition programming from the literature, and through interviews with external experts (see Figure 6). We then applied this framework to help identify the key success factors influencing the portfolio’s nutrition programmes.
Figure 6: Enabling factors that influence the effectiveness of nutrition programming

Strengthening political and technical coordination (across partners and government) was the most prevalent enabling factor, for eight out of 12 programmes. In countries such as Bangladesh, the DRC and Zambia, this was important for achieving consistency of nutrition service delivery, comprehensive population coverage and/or co-located services. For around one third of programmes, ineffective coordination mechanisms were a major constraint.
Securing political leadership and commitment was a key enabling factor for seven out of 12 programmes. A strong example of this is found within the Tackling Maternal and Child Undernutrition Programme in Zambia, where strong political commitment was in place at the national, district and village levels (including down to chiefs and village heads). For some other programmes, a combination of weak government and fiscal crises – leading for example to non-payment of health worker salaries and low motivation – presented significant programme constraints on effectiveness.
Five out of 12 programmes benefited from strengthening national and local capacity to deliver nutrition services. Working to Improve Nutrition in Northern Nigeria and programmes in Zambia provided training and technical support to community health workers and other volunteers (for example in growth monitoring, and the promotion of infant and young child feeding practices), which improved the quality of services. Despite these efforts, weaknesses in delivery capacity, including underfunded and overburdened health care systems and community volunteering structures, were still major constraining factors for some programmes, including in Nigeria and Zambia as well as Ethiopia.
External experts highlighted DFID’s evaluation and learning systems as a further success factor. ICAI found that most of the portfolio’s nutrition programmes demonstrated flexibility in response to changes in their context or evaluation evidence. Examples of adaptive management included flexible and rapid response to new humanitarian emergencies and crises (for example treating cases of acute malnutrition during the recent flooding in Zambia’s Northern Province, and in response to COVID-19 in Ethiopia), cost extensions to support the scale-up of services, and the incorporation of nutrition-sensitive components to help increase impact. Conversely, one third of programmes reported inadequate monitoring and evaluation as a constraining factor – including limited data systems to help identify, track and reach target groups, and to supply data on undernutrition.
Most constraining factors, however, related to external threats, including protracted environment and climate-related shocks, conflict and extreme poverty (reported by 11 out of 12 programmes). Shocks exacerbate periodic outbreaks of acute malnutrition, make access to the most vulnerable groups difficult (including when communities are displaced), and divert resources from longer-term activities. For example, the 2016 drought in Ethiopia, resulting from the El Niño weather effect, placed delivery pressures on most of the nutrition programmes reviewed. The Somalia country office flagged that working within an environment where both famine risk and ongoing conflict are daily challenges has placed severe pressures on its nutrition programmes.
Successful DFID nutrition programmes worked to mitigate these risks. ICAI found that DFID’s nutrition team played an important role in supporting country offices to improve their effectiveness, for example through sharing evidence of “what works”, as well as through the centrally managed Technical Assistance for Nutrition programme. The central-country team relationship is particularly strong in this area of programming. However, the nutrition team has had limited capacity, and inevitably it has not been possible to provide sufficient support across all areas.
Summary
Reporting against the reach target helped to maintain a strong focus on nutrition within DFID. The introduction of the intensity classification responded well to the 2014 ICAI review and has driven a greater focus on delivering quality nutrition programmes and a more comprehensive, evidence-based approach. DFID’s reported global result of 50.6 million women, children under five and adolescent girls reached through nutrition programming from 2015-2019 is credible overall, given the significant reductions to avoid double-counting. Most programmes within the nutrition portfolio have been achieving their immediate objectives and delivering positive nutrition outcomes. Successful programmes are underpinned by effective coordination mechanisms, political commitments to nutrition, increased local delivery capacity and adaptive approaches based on strong evaluations.
The emphasis on reporting reach risks underplaying the nutrition portfolio’s significant contributions to nutrition systems strengthening. The complexity of the results methodology, and variable statistical capacity within DFID, led to some inaccuracies in reported programme results. Errors were not always spotted in a timely manner. Evidence of positive outcomes is less consistent for nutrition-sensitive programmes, although primarily because relevant outcomes have not always been measured. DFID could have done better at systematically collating and sharing internally and externally the lessons from these programmes. Climate and conflict-related shocks are major constraining factors for programme effectiveness, alongside poor data systems and government funding constraints.
Equity: Are DFID interventions reaching the most vulnerable and hard-to-reach women and children?
DFID targeted locations where people are highly vulnerable to undernutrition
DFID’s Nutrition Position Paper states that the department will reach the “extreme poor, the most marginalised and those in fragile and conflict-affected states”. Evidence from the Lancet Series and other good practice (highlighted in ICAI’s literature review) suggests three necessary steps for targeting nutritionally vulnerable individuals. These are geographic targeting on the basis of poverty and food insecurity, community-based identification of households with nutritionally vulnerable groups (including women of childbearing age), and identifying and reaching the most marginalised individuals within these target groups.
Other donors, external experts and non-profit organisations agreed that DFID focused its attention on the right countries and the right areas within countries to reach the most vulnerable households. Africa and Asia bear the greatest burden of undernutrition, with more than half of all stunted children living in Asia, and more than one third in Africa. The bilateral nutrition programmes are predominantly targeting these regions, although with a greater focus on Africa (see Figure 7). Fifteen countries are targeted in Africa and three in Asia. This reflects DFID’s traditional general patterns of investment, but also projections that stunting will grow fastest in Africa, exacerbated by conflict and climate change.
Figure 7: DFID’s nutrition results by region (percentage split 2018 and 2019)
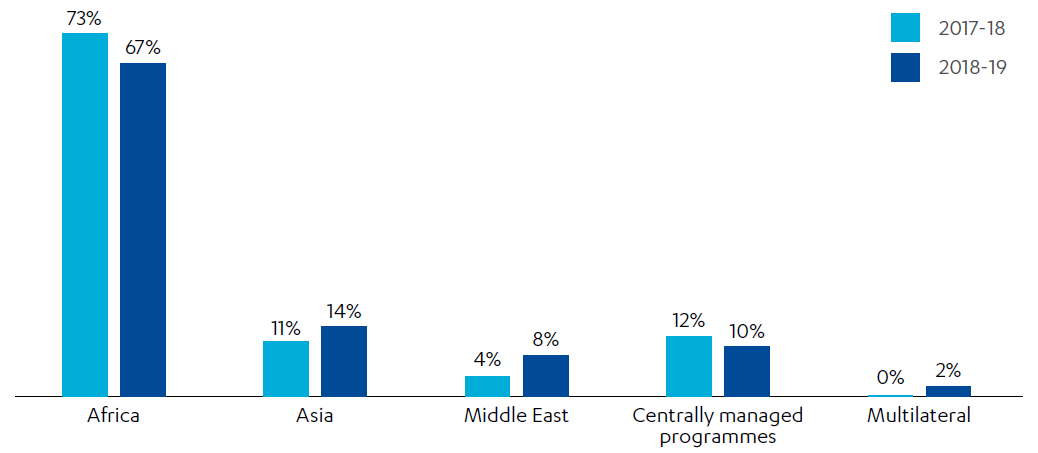
Source: Single Departmental Plan – Results Achieved by Sector in 2015-2019: Nutrition, DFID, 2019
In 2019, DFID reported that 49% of its nutrition results were from ‘high fragility’ countries and 37% from ‘fragile countries’. In fragile and conflict-affected states, the average prevalence of childhood wasting is 11.8% (compared with 8.9% in low- and middle-income countries) and stunting 37% (compared with 25%). The Integrated Food Security Phase Classification (IPC) classifies country populations by different levels of food insecurity. In 2019, 135 million people were in the ‘crisis’ phase or worse across 55 countries or territories. Bilateral programmes in 16 of these 55 countries have contributed to DFID’s nutrition results (from 23 DFID countries overall). Figure 8 displays the 55 countries judged to have the worst food crises in 2019 (IPC classification of three or higher) and those countries contributing to the nutrition portfolio’s results.
Figure 8: Countries with the worst food crises and their contribution to DFID’s nutrition results (2019)
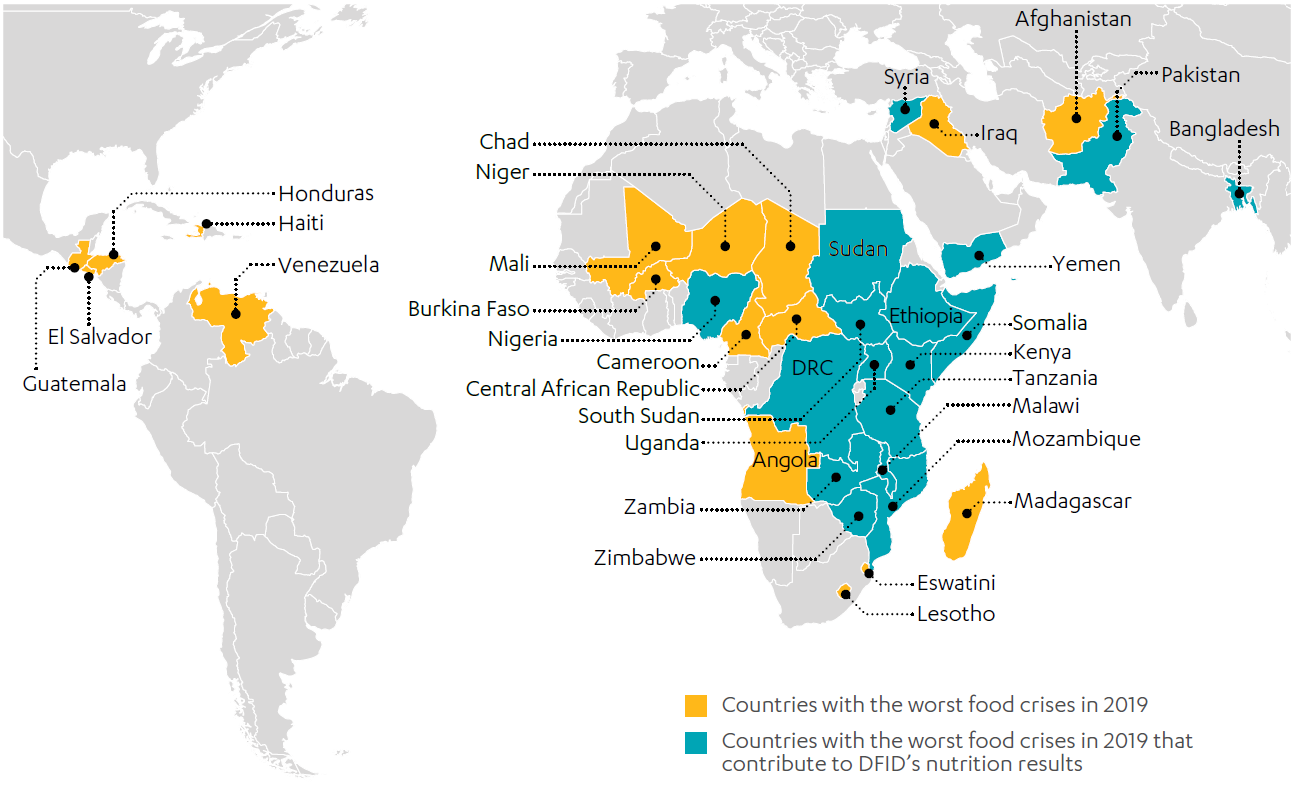
Source: Graphic created using data provided by DFID and data included in: Global Report on Food Crises: Joint Analysis for Better Decisions, Food Security Information Network, 2020
Within its target countries, DFID has implemented nutrition programmes, and in some cases focused its interventions entirely in localities where people are most vulnerable to undernutrition. DFID often undertook needs assessments to support this. Programmes in the DRC, Ethiopia and Tanzania targeted regions with the highest rates of stunting. In Kenya, the Hunger Safety Net Programme targets the four counties in Kenya with the highest poverty levels and greatest vulnerability to drought and floods. Further evidence of chronic food insecurity and rates of acute malnutrition exceeding emergency thresholds (greater than 15% of children under the age of five) influenced the location of the programme. The Zambia country team used the IPC assessment to target those populations worst affected by climate-related shocks, while Phase 2 of the Tackling Maternal and Child Undernutrition Programme targets districts based on high levels of stunting and poverty indicators from national data.
In such environments, the need for nutritional support is extremely high among the target groups. The problems faced were highlighted by citizens living in Zambia’s drought-stricken Western Provinces:
“In terms of agriculture, people were barely surviving because of the drought that hit this area. And most people have left their fields without being able to harvest anything…”
Focus group participant, Shangombo District, Zambia
“Here in the villages most of the children go the whole day from morning to evening without eating anything… sometimes you go three days without eating.”
Focus group participant, Sioma District, Zambia
DFID made significant efforts to reach the most vulnerable households through its programmes
ICAI was impressed by the varied strategies for reaching vulnerable households employed by the portfolio’s nutrition programmes. These involved building on and strengthening existing community structures, as well as developing pragmatic solutions within the context of poor or non-existent data systems. DFID and its delivery partners have relied heavily on community workers (both health workers and workers in other sectors) and volunteers to reach the most vulnerable households. It is generally recognised that community health workers, through integrating nutrition services within health services and implementing interventions at scale, are able to improve nutrition outcomes among hard-to-reach populations. Examples of this approach are outlined in Box 9.
Box 9: Approaches to community-based targeting of vulnerable households
- The Tackling Maternal and Child Undernutrition Programme in Zambia has used multiple community structures to identify and reach the most vulnerable households. District Nutrition Coordinating Committees plan and organise a package of nutrition services, with the aim of achieving convergence of these services, before drawing on ward-level delivery capacity including community health partnerships, safe motherhood action groups, and infant and young child feeding volunteers. The volunteers help with screening nutritional status and teaching community members about food preparation (through drama and demonstrations), either at the local health centre or through outreach to households. A community discussion in Mbala, Zambia highlighted how this combined model of using centralised health facilities with community volunteers travelling direct to households is an effective one. During fieldwork in Zambia, ICAI observed first hand DFID’s ability to reach its target groups with nutrition services (although not always the hardest to reach within its target groups), including in very remote areas such as Kasumalunga in Luapula Province. However, it should be noted that ICAI was only able to conduct fieldwork involving citizens in a limited number of areas in Zambia. The review team observed similarly effective outreach models involving volunteers in northern and southern Ethiopia.
- For the Productive Safety Net Programme in Ethiopia, eligible households are selected using a combination of objective data and participatory approaches. Initially, those districts which receive recurrent humanitarian food aid are identified. Within these districts, a panel of community members then selects a shortlist of households for targeting, using a checklist of eligibility criteria developed by the government. The provisional list is then discussed among the community and the final list is publicly posted. Those who feel that they have been wrongly excluded can apply to have their case reviewed by an appeals committee. Social protection programmes in Kenya and Zambia use data from proxy means tests to identify the most vulnerable households, predicting eligibility based upon observable characteristics proven to correlate with food insecurity.
- In Somalia, the nutrition programme has been providing assistance during ongoing climate and conflict-related crises that threaten the nutritional status of the most vulnerable. Due to the lack of capacity within the Somali government to deliver nutrition services, programmes deliver vital services to the most vulnerable through consortiums of national and international actors. For the Multi-Year Humanitarian Programme, the consortium also drew on community workers and mother-to-mother support groups to help identify the most vulnerable households (and provide training in child feeding).
The nutrition portfolio has been reaching vulnerable women and children under five, including in the most challenging environments
Target groups – children under five, women of childbearing age and adolescent girls – closely align with the evidence on who is most vulnerable to undernutrition, as well as where investment will bring the greatest benefits to society and the economy (through targeting the first 1,000 days of a child’s life). Infants, young children and women of childbearing age are most vulnerable to undernutrition as their bodies have a greater need for nutrients, such as vitamins and minerals, and are more susceptible to the harmful consequences of deficiencies. The 2008 Lancet Series on maternal and child nutrition identified the need to focus on the period of pregnancy and the first two years of life (the first 1,000 days). After the age of two years, undernutrition will have caused irreversible damage for future development towards adulthood.
ICAI also found that the target groups of pregnant and lactating women and children under five have been clearly established within the logframes of programmes contributing to nutrition results. Because of this, some programme partners, including other donors and non-profit organisations, consider nutrition to be an area of the department’s programming with a particularly strong pro-poor and gender focus.
“We will increase our work to address the needs of young children, particularly focusing on the first two years, to prevent stunting, wasting and micronutrient deficiencies. We will also put girls and women at the heart of our work on nutrition, particularly targeting unequal access to food, water and other essential services.”
The UK’s Global Nutrition Position Paper, DFID, 2017, p. 3.
In its global nutrition results, DFID reported exceeding its target to reach 50 million people (children under five, women of childbearing age, and adolescent girls). In 2019, 53% of those reached were reported to be women and girls, plus 16% were boys under-five. The gender of 31% of the portfolio’s nutrition results is unknown, often due to a lack of disaggregated gender data collected through government systems, or through DFID’s own programme monitoring in cases such as low-intensity mass communication campaigns. Gender-disaggregated data is expected to be provided for this type of programme in future.
ICAI assessed most of DFID’s nutrition programmes within the review’s sample as either effective or highly effective in reaching vulnerable women and children. This was based upon data showing that programme targets to reach these groups had been met, as well as evaluation and other evidence. In Ethiopia, ICAI found that midwives made concerted efforts to work around women’s time burdens and household responsibilities, for example by fitting appointments around market times or making them as short as possible. In Zambia, volunteers provided tailored counselling based upon the needs of different members of the household. In Zambia’s Lunga and Mongu Districts, citizens noted that community-based volunteers visited monthly, were helpful and responded to the concerns of young mothers:
“We take the child to the clinic- there they will give us the medicine and advice on the food we should give to that child – and continue taking the child for check-ups.”
“They teach us starting from when a person is pregnant up until when she delivers, the kind of food she is supposed to eat so that the unborn baby can grow well and for the mother not to have any complications during childbirth.”
Focus group participants, Mongu District, Zambia
The constraining environments in which the portfolio’s nutrition programmes have operated made it extremely challenging to provide services to vulnerable groups. Despite this, several interventions demonstrated impressive results, for example in reaching women and children suffering from malnutrition in crisis contexts.
- In Somalia, through the Multi-Year Humanitarian Programme, 361,966 children aged under five and pregnant and lactating women received ready-to-use therapeutic foods between 2013 and 2017, and 89,008 children were admitted for treatment.
- Through the Building Resilience in Ethiopia programme, UNICEF reported that it helped treat 60,814 children under five for acute malnutrition through ready-to-use therapeutic food products, following an internally displaced people crisis, and achieved a treatment success rate of over 90%. More recently, the programme has helped to provide a flexible response to the COVID-19 pandemic, reaching an additional 100,000 malnourished children with nutrition support.
- In 2016-17, emergency cash transfers under the Zambia Social Protection Programme reached 20,568 of the most vulnerable households in hard-to-reach locations during a severe drought caused by the El Niño weather pattern. UNICEF flagged that DFID Zambia was the only donor funding the procurement of ready-to-use therapeutic food products (through the Health Systems Strengthening Programme), to help treat acute malnutrition among the most vulnerable.
ICAI was told by local citizens in Amhara, Ethiopia, that without interventions such as the Productive Safety Net Programme, more vulnerable people would probably have migrated from the community and been exposed to greater risks. Citizens reported that the programme had supported women and children to access and increase their household consumption of nutritious foods, both through direct food transfers and through supporting small-scale agriculture and livelihoods projects through public works. The latter also helped families to pay for school fees and clothes. Similarly, DFID’s emergency food relief programme in Zambia was recognised by citizens living in the worst affected areas as providing a lifeline:
“Before the food distribution, we only ate once a day. We ate reeds, weeds – these are foods that were dirty and not nice to look at.”
“Before the programme reached our village, things were bad … some children almost ran away from their villages to go live with other people … We are thankful to this programme; it has brought back friendship among us people in the village.”
Focus group participants, Shangombo District, Zambia
DFID did not fully understand and always reach the most marginalised within its target group
The 2014 ICAI review stated that DFID should specifically ensure that its interventions better target the nutritional needs of the most vulnerable mothers and children, in order to meet ‘leave no one behind’ commitments. However, beyond the broad goal of reaching 50 million women and children, there are no further disaggregated targets for these or other vulnerable groups (for example people with disabilities or chronic disease). It would be extremely challenging for country teams to report against further disaggregated targets, given weaknesses in government data systems and the department’s reliance on partners to collect this data.
To have an impact on nutrition, the portfolio’s programmes also aim to maximise coverage of the target group (to 90% of the population). This means that there is less of an incentive for nutrition programmes to develop specific targets and engagement strategies for the most marginalised. ICAI found that the targeting of adolescent girls, for example, was less evident. Only three programmes had targets to reach people with disabilities. Even fewer were monitoring disability. Due to this and the quality of programme and national data systems, the availability of disaggregated monitoring data has also been highly variable, even for gender. Because of this, DFID did not always know exactly who it had reached. One positive exception was the Access to Healthcare programme in DRC, where DFID made strong efforts to reach people with disabilities across the target areas, and health facilities were required to report this information using the district health information system.
DFID had also not developed a deeper understanding of who the most vulnerable were and how to reach them effectively. ICAI found a lack of analysis on the characteristics of the most vulnerable as well as specific research into understanding their needs, for example covering the underlying causes of undernutrition, or their drivers and barriers to service engagement, at country and programme levels. Linked to this, there was a lack of detailed guidance from DFID on how to engage the most vulnerable in nutrition programmes (for example strategies for different sub-groups of vulnerable women, which take into account women’s household and livelihood activities). This is despite evidence of recurring challenges. The 2014 ICAI review also found that projects needed to be tailored to help better target the most vulnerable and hard to reach.
In practice, ICAI found that the interventions have not always reached the most vulnerable and hard to reach within communities. In Zambia, vulnerable groups that were reportedly not being consistently identified and engaged (through the Tackling Maternal and Child Undernutrition Programme) included female-headed households, households headed by a disabled or chronically ill person and child-headed households. In Ethiopia, programmes faced difficulties in reaching nomadic pastoralist communities, as well as women who migrated from rural to urban areas outside of the harvest. In the poorest rural communities, weak transport links create difficulties in accessing services, and programmes have also faced cultural barriers to service uptake among young mothers. An impact evaluation in Nigeria found that target groups had been reached by DFID, but it noted that mothers from the poorest households and from households furthest away from health facilities, adolescent mothers and mothers with no formal education were less likely to be reached. This was despite the programme making a concerted effort to take services to the hardest-to-reach households using mobile nutrition teams.
Two promising resources shared with partners during 2019 (through the Technical Assistance for Nutrition programme) included: (1) a systematic review of the relationship between disability and malnutrition and (2) a DFID-commissioned knowledge product on how to integrate a disability lens into nutrition programming. The Technical Assistance for Nutrition programme has the potential to enable a better understanding and targeting of the most vulnerable groups, including the hardest-to-reach women, in ways that include sharing lessons across nutrition programmes.
The nutrition programmes have supported national civil society alliances to inform policy and planning on nutrition and to promote greater citizen accountability, including through the department’s funding to the SUN Movement. ICAI found, however, that alliances were more active in some countries than others. ICAI also saw a need for strengthening feedback mechanisms at the community level, to help ensure that the voices of the most marginalised are listened to, understood, and could inform the nutrition programmes. When we conducted a group discussion with citizens accessing the Productive Safety Net Programme in Seqota, Ethiopia, the selection criteria for inclusion in the programme were not clear to all participants, further suggesting the need for improved citizen engagement. ICAI heard similar feedback in Zambia, in relation to the Health Systems Strengthening Programme:
“…what about us who are not on the programme but are also as vulnerable as the others? We also want to be on the programme and eat like the others … So, I would say that the process that was used to register people on this programme was not very clear. It is confusing because a lot of people seem to have been left out.”
Focus group participant, Shangombo District, Zambia
In Ethiopia, ICAI saw potential for ward-level nutrition committees, supported by the portfolio’s programmes, to conduct more outreach work to help understand the needs of the most vulnerable households, as well as for building on NGO-sector models of community participation. ICAI also found some positive existing examples of citizen consultation within the portfolio to build on:
- In Nigeria, the independent evaluation found that key success factors in increasing the number of pregnant women reached with iron folic acid supplementation included developing micro-plans and conducting community dialogues and the use of town announcers to help increase the demand for services.
- In Somalia, community resilience committees were used to create an action plan for nutrition services to target and reach the most vulnerable households, involving community members and overseen by service partners. These community committees then selected households through established criteria to receive direct support.
Wider barriers to reaching the most vulnerable include a lack of reliable data and coordination mechanisms, and capacity constraints on community workers and volunteers
Weak government data systems and the lack of accurate household-level data are a major challenge for the nutrition portfolio in targeting the most vulnerable. Under the first phase of the Tackling Maternal and Child Undernutrition Programme in Zambia, for example, DFID was not always able to identify the most vulnerable households due to an overreliance on district-level data, despite the support of community workers. ICAI found promising examples of data-driven targeting within the social protection sector, on which the nutrition programmes might build in future. The proxy means tests used to identify eligible households generate valuable disaggregated data on the most vulnerable in a community. Using these systems could also provide the basis for better planning for the convergence of services on vulnerable households. In countries such as Ethiopia, the department is providing longer-term support for strengthening government data systems, including the transition to electronic records, and improved monitoring and accountability of nutrition services.
ICAI also found that a lack of coordination mechanisms has hindered identifying and reaching the most vulnerable households. As we have seen, some programmes have supported the development of multi-sector ward and district nutrition coordinating committees, which in turn mobilise a range of community workers and volunteers. However, ICAI’s fieldwork highlighted how districts not included in Zambia’s Tackling Maternal and Child Undernutrition Programme (but falling under Zambia’s Health Systems Strengthening Programme) lacked similar committees to coordinate and deliver services.
Reflecting a finding from the 2014 review, ICAI heard during the country visits that some community workers and volunteers are becoming overburdened and face mounting capacity constraints as nutrition and other health programmes have expanded and diversified. In Ethiopia, the Health Extension Workers, considered a model of good practice in the region, are stretched across different services. This is despite this being a salaried governmental cadre, with supervision from local health facilities. In Zambia, primarily unpaid community volunteers shoulder the responsibility of reaching the most vulnerable, including carrying out important duties such as providing ready-to-use therapeutic food products to children with acute malnutrition, and administering follow-up treatment for several weeks in some of the worst climate-affected areas. Volunteers in both Zambia and Ethiopia highlighted the financial and social costs of volunteering, including, in Zambia, leaving their families for several days to reach remote households.
Within this context, reaching the most vulnerable households becomes highly dependent upon the availability of trained workers and volunteers and their motivation and abilities. This can produce mixed results. In Ethiopia, DFID said that nutrition services face challenges in reaching homes within more remote regions such as Somali and Afar, due to a lack of trained health extension workers and poor transport links. A group discussion with volunteers in Mbala, Zambia revealed how not all vulnerable households are reached because of the distances that volunteers must travel (sometimes over 5km on foot) and a lack of transport such as bicycles. In Zambia, ICAI heard reports from one district that using community workers and volunteers in contexts where there is the severest food insecurity has not always been effective. With the whole community experiencing hunger during crisis situations, outreach activities can be severely weakened. The limits of community outreach were raised by citizens in Shangombo District, Zambia:
“Because there are only a few people that are receiving this help, it becomes a problem… they cannot help everyone who goes to get help.”
“There are community workers in our area who are supposed to be teaching people on hygiene and how to use toilets, to keep the toilets clean and all, but these people are failing.”
“The volunteers are there… But they don’t work.”
Focus group participants, Shangombo District, Zambia
There is often overload and breakdown of systems that rely on very low-paid or volunteer workers. ICAI saw a need for governments and donors to strengthen their longer-term strategies for engaging and supporting volunteers in countries where they are integral to nutrition programming. The Zambia country office, for example, said that they are supporting the government of Zambia to operationalise a National Volunteers Policy, through their support to the UN Joint Programme on Social Protection. Volunteers in Zambia also suggested that listening more closely to their feedback would help the department to understand better how to work with volunteers and within existing community health structures, as well as what is required to identify and reach the most vulnerable groups.
Summary
DFID’s target groups aligned with the evidence on groups who are at high risk of undernutrition. The portfolio of nutrition programmes has targeted vulnerable women and children within countries (and areas within countries) that experience heightened food insecurity, often as a result of conflict and climate change. Despite operating in such challenging contexts, these programmes have effectively reached vulnerable households, and the primary target group of women of childbearing age and children, through working within existing community structures and with community health workers and volunteers. This contributed towards DFID exceeding its target to reach 50 million people (children under five, women of childbearing age, and adolescent girls), based on its nutrition results between 2015 and 2019.
The focus on maximising coverage of its target groups (in line with evidence from the Lancet Series), a lack of disaggregated targets, and poor data and monitoring systems hindered DFID’s ability to reach the most marginalised women and children. It is disappointing that DFID’s mechanisms had not significantly improved in this area since the 2014 ICAI review. There is a lack of research and guidance on how to increase engagement with the hardest-to-reach women, despite support being in principle available through programmes such as the Technical Assistance for Nutrition programme. Opportunities have been missed to build on existing poverty targeting systems, such as those used by DFID’s social protection programmes, to complement the work of community workers who are overburdened.
Impact: To what extent is DFID helping to reduce malnutrition?
DFID’s nutrition strategy and programmes were evidence-based with strong potential for impact
DFID’s nutrition portfolio has been aligned with best practice on reducing undernutrition. The literature states that a multi-sector approach, addressing both direct and underlying causes, is required to improve nutrition. The 2017 Nutrition Position Paper confirmed DFID’s commitment to a comprehensive approach, including mainstreaming nutrition through nutrition-sensitive programming working across sectors, partners and government ministries. Mainstreaming nutrition is the more effective and sustainable approach for governments.
The literature also emphasises the importance of ‘building an enabling environment’ for nutrition. DFID’s strategy therefore has balanced meeting the immediate needs of vulnerable populations with a longer-term focus on capacity-building government systems. It has also advocated for international and national leadership, to drive political prioritisation and investment in nutrition. This reflects evidence that achieving sustainable reductions in malnutrition requires high-level political ownership of the problem and that key factors hindering progress include weak service delivery systems and inadequate investments in nutrition.
The nutrition strategy and results methodology further align with the evidence in encouraging country teams to implement high-coverage and high-intensity interventions that ‘converge’ on the same vulnerable groups and households. Among external experts, working across sectors is widely agreed as key to achieving global reductions in malnutrition.
One strong example of DFID’s multifaceted approach has been its work on treating and preventing acute malnutrition. ICAI found that DFID had a clear focus within its nutrition work on responding to crises, such as droughts and conflict, as an important underlying driver of undernutrition. The programmes have provided timely humanitarian food assistance and management of acute malnutrition, often when the government (and other donors) are slower to respond. At the same time, the nutrition portfolio has supported longer-term social protection programmes that address the underlying drivers of chronic poverty and food insecurity. These programmes aim to reduce the need for short-term and more expensive humanitarian intervention through supporting household consumption outside of the harvest season. Programmes also aim to build the capacity of government to manage social protection systems and better anticipate food crises.
ICAI found that 18 out of 20 nutrition programmes were strongly informed by evidence of “what works”, increasing their likelihood of being impactful. Country teams have been prioritising nutrition-specific interventions where there is the strongest evidence of impact, alongside nutrition-sensitive programmes and approaches that are more broadly evidence-based, to help address the multi-dimensional causes of undernutrition. Countries which support both, for example Ethiopia, Zambia and Tanzania, most closely align with the evidence of what is needed to reduce undernutrition sustainably. Furthermore, of the 20 programmes reviewed by ICAI, 13 programmes had a strong and explicit focus on strengthening systems and the capacity to deliver equitable nutrition services (and six programmes a more moderate emphasis).
Some external experts expressed concern that the department should not move too far in the direction of nutrition-sensitive programming, given that the evidence of impact is still the strongest for nutrition-specific interventions. Other experts questioned the inclusion of low-intensity results altogether – nutrition-sensitive programmes not specifically directed towards target groups – on the basis that they might not improve nutritional status. Overall, ICAI found that stronger guidance would be beneficial on what constitutes nutrition-sensitive programming (across different sectors), what has most impact, and how such programmes contribute to ‘intermediate’ nutrition outcomes (such as improved quality of diets and disease burden) and can be measured.
The programmes are making progress on strengthening global and national leadership and action on nutrition
Other donors which have worked with DFID and external experts consider that DFID made important contributions to influencing a greater focus on nutrition globally. This was achieved through helping to convene international partners at global summits, supporting advocacy and technical assistance through the SUN Movement, and encouraging the increased resourcing of nutrition through DFID’s own financial contributions. In these ways, DFID helped to create collective momentum towards achieving the global nutrition targets. This builds on progress in this area noted in the 2014 ICAI review. External stakeholders consider that DFID provided further leadership on equity, through influencing a focus on marginalised groups across the nutrition sector. This is reflected at country level, where DFID often encouraged the involvement of gender ministries in cross-sector policy discussions.
The 2014 ICAI review found that DFID had made good progress in building government delivery capacity. In most of the eight countries reviewed by ICAI, DFID made further progress towards building political leadership and commitments to nutrition, working with country governments. For example in Zambia, DFID had become a key cooperating partner with the government and has helped to ensure that nutrition is a national priority, supported by a National Food and Nutrition Strategic Plan. In 2018, at a National Nutrition Summit convened with support from the UK and other partners including UNICEF, the Zambian vice president announced a government commitment of 400 kwacha (£17) per child per year for nutrition. In Nigeria, an impact evaluation found that DFID had significantly increased political commitment to fund nutrition at the federal, state and local government levels. Globally, the Technical Assistance for Nutrition programme has been instrumental in countries adopting nutrition-specific and nutrition-sensitive interventions.
In these countries, DFID’s advocacy and technical assistance also contributed to the longer-term integration of nutrition within government services and programmes. DFID made progress in supporting the mainstreaming of the nutrition-specific package into basic health care services in Ethiopia and Nigeria (including vitamin supplementation and community management of acute malnutrition), as well as nutrition-sensitive components into social safety net systems in Ethiopia, Kenya and Zambia.
DFID also made some progress in influencing increased financing for nutrition – most notably in Ethiopia, Nigeria and Tanzania. Through building strong relationships with government, DFID’s programming in Nigeria led to an increase in the budget allocation for nutrition in target states (from zero to 3 billion naira, or £6 million), as well as the inclusion of ready-to-use therapeutic food products in the country’s essential medicines list. With support from DFID and UNICEF, the government of Tanzania established a Nutrition Compact between central and local authorities, to encourage a minimum level of spend per child under five, and committees to oversee multi-sectoral nutrition interventions at national, regional, district, ward and village levels.
However, the aid programme is often working in countries with constrained fiscal environments. Financial commitments to nutrition continue to be insufficient relative to the scale of the problem. In Tanzania, for example, the Nutrition Compact commits to spending 1,000 Tanzanian shillings per child (£0.30), when the international recommendation is £7 per person. DFID also found that disbursements across district councils, and levels of accountability, varied. Similarly, greater progress is needed on improving national data systems, as noted throughout this report, to help improve the ability of agencies to identify and track the most vulnerable.
The portfolio is likely to deliver longer-term impacts on undernutrition, although recent progress on reducing stunting and wasting has been mixed
Overall, the nutrition portfolio has the potential to impact on reducing undernutrition over the longer term (assuming that its programmes are sustained). This is based upon DFID’s evidence-based approach, commitment to partnerships and systems building, and the positive results from its programmes.
DFID’s impact should be viewed in the light of mixed global performance on reducing undernutrition (as measured by rates of stunting and wasting). Positively, many of DFID’s target countries have seen long-term decreases in stunting. In Bangladesh, Ethiopia and Zambia there have been significant improvements. Stunting decreased in Ethiopia from 50% to 37% between 2005 and 2019. However, in more recent years, progress has begun to plateau (see Figure 9). Intractable problems of undernutrition remain within some areas and groups of people, due to deep structural inequalities.
Figure 9: Progress in reducing stunting in Tanzania and Ethiopia (percentage rate among children under five)
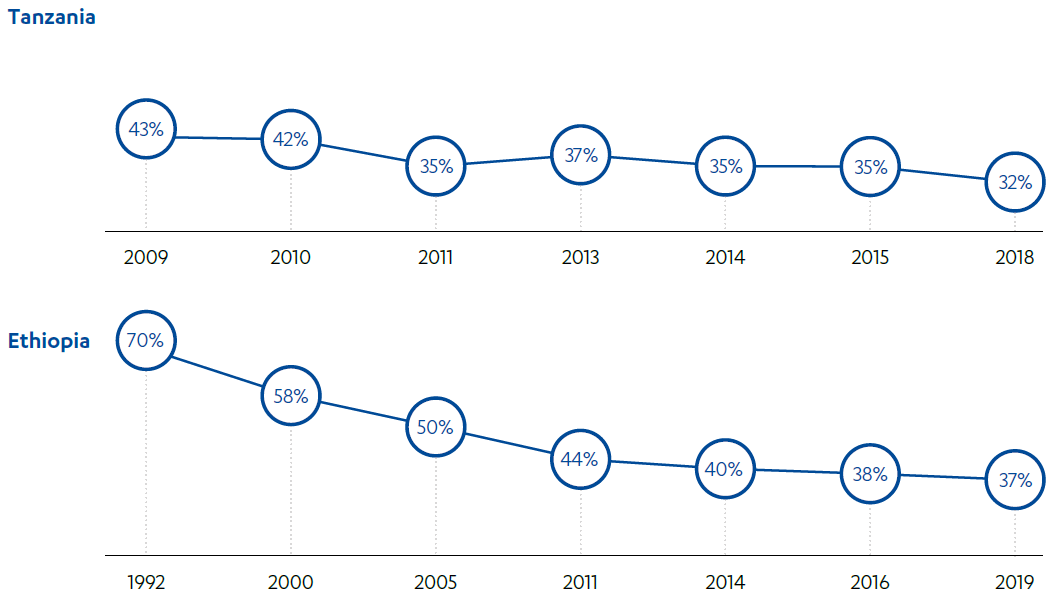
Source: Graphics created using data from: Prevalence of undernourishment, The World Bank, link. Data for Tanzania is derived from two different national surveys.
In the poorest and most fragile countries within our sample, the prevalence of malnutrition has not improved at all. In Nigeria, figures highlight a fluctuating and overall negative trend (see Figure 10). The prevalence of acute malnutrition has remained at levels of 5-10% since 2014. In Somalia, malnutrition cases have remained high (at around 300,000 per year) for over a decade, exacerbated by recurrent crises.
Figure 10: Progress in reducing stunting in Nigeria (percentage rate among children under five)
Source: Graphic created using data from: Prevalence of undernourishment, The World Bank
The challenging context for improving nutrition among the most vulnerable populations is reflected in the mixed level of impact reported by DFID’s programmes. ICAI assessed programme impact using a variety of sources – although the availability of relevant impact evaluations was key. For six programmes where relevant data was available (13 overall), ICAI found evidence of mixed to positive levels of impact on undernutrition. These programmes reported reductions in stunting (although no more than 5%) as well as wasting. However, reductions tended to be less than anticipated in logframe targets and wasting tended to be harder to shift than stunting.
Box 10: Impact of nutrition programmes in Zambia
In Zambia, the evaluation of the Tackling Maternal and Child Undernutrition Programme (2013-18) found promising evidence of a reduction in stunting among children aged six to 23 months (who were more likely to have had exposure to the programme). This data was reflected in findings from ICAI’s fieldwork and consultation with local citizens:
“Those days children would suffer from diseases due to poor feeding but these days it’s no longer the same; the children are fed properly and malnutrition cases have decreased because of the information we received from the project – we now know how to handle our children and protect them from diseases.”
Focus group participant, Mongu District, Zambia
In 2018-19, the Health Systems Strengthening Programme provided interim food relief before Phase II of the Tackling Maternal and Child Undernutrition Programme started. This was also recognised by citizens to be life-saving:
“If it were not for them [food relief services], I personally would have died, and I speak for everyone here.”
Focus group participant, Shangombo District, Zambia
However, while the impact evaluation of the Tackling Maternal and Child Undernutrition Programme found a 4 percentage point decrease in stunting among children under five in the intervention districts (and there was a 5% reduction nationally by 2018), unsurprisingly it was not possible to attribute this entirely to the programme. In Zambia, the prevalence of stunting remains stubbornly high in the targeted Central and Western Provinces, at up to 46% compared with 37% nationally.
Seven programmes reported no change or a decline in measures of undernutrition such as stunting or (in the case of Zambia’s WASH programme) limited reductions in diarrhoea. Examples include the following:
- The impact evaluation of Working to Improve Nutrition in Northern Nigeria found that, despite ambitious targets to reduce stunting and wasting by 20%, there were no significant changes among children under three years from baseline to endline in treatment areas, and that in some cases levels worsened. This was attributed to a lack of complementary nutrition-sensitive interventions, low geographical coverage, and insufficient time for impact to be detected.
- The evaluation of Zambia’s Social Protection Expansion Programme reported positive impacts in core areas, including a 10 percentage point reduction in poverty in target districts, but noted no impacts on most child health and nutrition indicators. This was attributed to factors beyond the control of the intervention, including “the supply of social services and infrastructure such as education, health care, and access to clean water”.
External factors constrained these and other DFID nutrition programmes from being impactful. In countries such as Ethiopia, Somalia, Nigeria and the DRC, periodic droughts and conflict coincided with the period covered by DFID’s nutrition results. The DRC continues to experience a protracted civil war, which has led to a large-scale nutrition crisis, resulting in 770,000 malnourished children (440,000 of whom still urgently need treatment for severe acute malnutrition). Due to conflict, DFID’s programme activities were suspended in one region for nine months, and only resumed once people returned to their villages. An understanding of the underlying determinants of undernutrition, alongside more recent evidence on nutrition-sensitive agriculture programmes, suggests that it is unrealistic to expect such programmes to impact on stunting and wasting on their own due to multiple confounding factors. Instead, nutrition-sensitive agriculture programmes should focus on and measure changes in the underlying causes of malnutrition, such as access to and consumption of high-quality diets. This also strengthens the case for promoting the convergence of nutrition-sensitive and nutrition-specific interventions on the same at-risk populations.
For seven programmes, there was insufficient evidence for ICAI to determine impact. Most of these programmes were not monitoring impacts on nutrition and did not have an impact evaluation with a nutrition focus. For three of these programmes, where the primary aim was to strengthen national systems and capacity, it would be more appropriate to measure impact over the longer term. Nonetheless, these programmes did not yet have sufficient plans in place to assess this. For the Technical Assistance for Nutrition programme, processes to gather systematic evidence of systems impacts (such as increased government ownership, allocation of resources and coverage of nutrition services) were not instituted at the outset and are only gradually being introduced.
In all cases it is difficult to attribute country-level changes in undernutrition to DFID’s portfolio. There is a lack of national-level evaluation studies that assess the contributions of different nutrition actors. The impact of the UK’s programmes will inevitably vary depending upon the context of government resources and other donors operating in nutrition. In countries such as Bangladesh, which has seen the second highest reduction in stunting among ICAI’s sample, and where DFID and its partner BRAC were delivering one of the largest nutrition portfolios in the country (working closely with and complementing the government’s health and nutrition services), DFID estimated that progress would have been half this rate without its interventions. ICAI however was not able to verify this claim. In those countries suffering from humanitarian crises (and given the evidence of positive results from DFID’s programmes) the UK nutrition portfolio has arguably helped to prevent the situation from worsening, for example in Somalia.
Longer-term, from the 20 programmes assessed, 13 were judged by ICAI to have the potential for some impact and six for high impact. Six country portfolios were judged to have the potential for some impact, and two for high impact. Likelihood of less impact was associated with a weaker focus on systems building, or else insufficient support for the convergence of multi-sector interventions that tackle the underlying drivers of undernutrition.
UK aid’s nutrition programmes have faced multiple underlying constraints to reducing stunting and wasting. These include extreme poverty and food insecurity (particularly where safety nets were not available), cultural barriers to service uptake and behaviour change, weak health delivery systems, adolescent pregnancy, insufficient WASH facilities, poor transport infrastructure, and limited local access to nutritious foods. Such factors in turn weaken the resilience of communities to recurrent shocks and crises. Within this context, some nutrition programmes found that they were overambitious with their impact targets (such as to reduce stunting by 20%). Tackling the complex and longer-term processes involved in shifting intergenerational malnutrition, as noted by the DRC country office, requires stronger multi-sector efforts.
The multi-sector approach to nutrition is still under development particularly in food systems
ICAI found that the nutrition portfolio’s multi-sector approach is still work in progress. Most of DFID’s nutrition activities have been focused within the health, humanitarian and social protection sectors. Figure 11 provides an indication of the split of activities by sector, based upon DFID’s nutrition-related programmes in 2017.
Figure 11: Sector activities in nutrition interventions
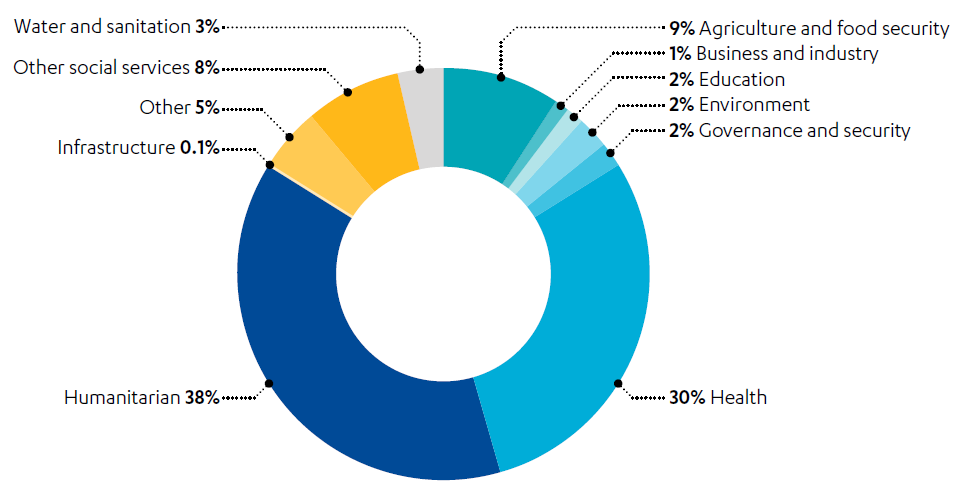
Source: Based on counts of different programme components relating to each sector, rather than expenditure. Graphic created based on data from DFID’s aid spending for nutrition: 2017, Development Initiatives, 2019.
Similarly, while country nutrition portfolios demonstrate commitments to a multi-sector approach, ICAI found that they are still under development. DFID (and its partners) have not been sufficiently addressing some of the underlying causes of undernutrition. ICAI found that DFID was learning from this experience. The Ethiopia country team has been exploring how other sector programmes, including WASH and agricultural development, can be made more nutrition-sensitive, and has commissioned MQSUN+ to review its portfolio. In Nigeria, the evaluation of the Working to Improve Nutrition programme attributed limited impact to a lack of complementary nutrition-sensitive interventions (alongside the programme’s nutrition-specific package) – DFID subsequently incorporated income-generating activities. Phase II of the Tackling Maternal and Child Undernutrition Programme in Zambia has been planned to include an intervention on Dietary Diversification through Nutrition-Sensitive Agriculture, on the basis that this will increase impact on stunting and wasting.
At the central level, the department has recently finalised useful nutrition value for money guidance, which lists nutrition-specific and nutrition-sensitive interventions with strong existing evidence of impact and cost-effectiveness. It would be useful to develop this further, to identify what works for nutrition-sensitive programming, why and in what contexts (including when combining interventions), for example through detailed case studies. This could help to inform programme design and accelerate achieving the ‘nutrition boost’ across different sectors.
External expert stakeholders, including other donors, academics and SUN partners, reflected that DFID was still learning how to work effectively across their country portfolios in support of the required multi-sector approach. Some argued that an increased emphasis is needed on the integration of nutrition within work on food systems and resilience to climate change. This involves strengthening the role of climate-smart agriculture and private sector development in improving access to affordable, sustainable and nutritious diets.
Box 11: Understanding food systems
The UN’s Sustainable Development Goals advocate for major transformations in agriculture and food systems in order to end hunger, achieve food security and improve nutrition by 2030. Food systems are defined as “the entire range of actors and their interlinked value-adding activities involved in the production, aggregation, processing, distribution, consumption and disposal of food products that originate from agriculture, forestry or fisheries, and parts of the broader economic, societal and natural environments in which they are embedded.” A sustainable food system can be defined as “a food system that delivers food security and nutrition for all in such a way that the economic, social and environmental bases to generate food security and nutrition for future generations are not compromised.” Recent evidence from the Lancet highlights that transforming food systems is essential for supporting the health of people and the planet, and that undernutrition and overnutrition must be tackled together to address the double burden of malnutrition. To transform food systems, the High Level Panel of Experts of the Committee on World Food Security suggests action on multiple fronts, including (1) improving food supply chains, such as production of nutritious foods through environmentally friendly farming practices, improving connectivity between rural and urban areas, (2) improving the quality of diets, such as phasing out advertising and promotion of unhealthy foods, regulating food packaging, and (3) creating consumer demand for nutritious food, such as guidelines for healthy diets, tax policies on foods of differing nutritional value.
Food systems have been a focus for DFID since the 2013 Nutrition for Growth Summit. In 2014, DFID established the Global Panel on Agriculture and Food Systems for Nutrition. The Panel is an independent group of leaders who have shown commitment to nutrition, and aims to influence policymakers from different sectors in the food system. For the multilateral Global Agriculture and Food Security Programme, DFID played a leading role in encouraging a revised monitoring and evaluation framework, which enables the programme to track progress on improving the minimum dietary diversity of women and children. DFID’s nutrition team noted that greater progress is needed on engendering support for nutritious food systems across multilateral institutions, and within country governments. We were told that food systems (alongside health systems and climate change) would be a priority focus for DFID at the next Nutrition for Growth Summit.
DFID responded positively to the 2014 ICAI recommendation that it should “explore how to effectively engage the private sector in nutrition”. The 2017 Position Paper outlines DFID’s aim to “mobilise greater private sector investments in agriculture and food systems that improve the quality of diets for women, adolescent girls and children”. ICAI also found examples of DFID adding a nutrition boost to its agriculture and economic development work across three types of activity:
- Programmes have helped farmers to improve nutrition and increase their incomes by switching to nutritious crops, for example in Bangladesh. HarvestPlus was a global initiative to demonstrate the efficacy of biofortified crops, reaching 7.6 million households in nine countries. DFID reported that around a quarter of projects under the Adaptation for Smallholder Agriculture Programme, which channels climate finance to farmers, explicitly support improvements in nutritional status through combinations of support to nutritionally important crops and foods, as well as nutrition-specific training.
- DFID also incentivised seed companies, food manufacturers and retailers to make the switch to nutritious, biofortified crops, including through business grants. ICAI viewed three such businesses that the Zambia country team was supporting through the Private Enterprise Programme (which has also developed a ‘rural enterprise hub’ for local maize farmers). DFID said that it was funding similar schemes in Nigeria, Zimbabwe, Tanzania, Rwanda and Kenya. The West Africa Food Programme provided incentives to companies to produce affordable nutritious foods, sourced from smallholder farmers, and reported producing 34,000 tons of nutrition-fortified staple food products in the last two years of the programme.
- In Nigeria and Kenya, DFID reported that it was working with UK and African agri-tech companies to develop affordable solar-powered cold storage solutions and help increase the availability and reduce the cost of nutritious foods such as milk, fruits and vegetables. The Africa Food Trade and Resilience programme aims to address food shortages through regional food production, processing and trade, including in nutritious foods.
Despite this, ICAI found that food systems approaches were neither comprehensive nor fully integrated with nutrition plans at country level. In 2016, DFID committed to ensuring that new bilateral agriculture programmes included nutrition outcomes, and since then the number of such programmes has increased. However, while DFID’s most recent portfolio review counted 35 (or 71%) of 49 commercial agriculture projects aiming to deliver nutrition benefits, the majority related to increased household consumption (45% of all programmes), an indirect measure of nutrition, rather than improved dietary diversity or reductions in stunting (20% of all programmes). The latter would require a more comprehensive approach. Fieldwork in Zambia highlighted the weakness of the agriculture sector and the lack of investment in developing nutritious food systems for the growing population. In Ethiopia, support for private sector development and nutritious food systems is nascent, with the main area of relevant activity viewed by ICAI being small-scale agricultural public works within the Productive Safety Net Programme. In Nigeria, the lack of local food production and over-reliance on imported food compounds issues of food insecurity and malnutrition during periods of crisis. This was found to be a key constraint on DFID’s impact. While programmes for this review were sampled to include coverage of agriculture activities, few programmes had outputs related to the production of nutritious foods. Not all the programmes listed in the previous paragraph contribute to the UK’s nutrition results.
This gap was corroborated by citizen feedback in rural communities, who noted how better access to nutritious foods (and agriculture support) was their greatest area of additional need (alongside social protection services in Zambia and water and sanitation in Ethiopia). In the Amhara region of Ethiopia, citizens said that an increased supply of seeds and improved irrigation were required to help improve nutrition, alongside the social protection scheme and maternal and child health services in place. A focus group discussion in Zambia suggested that agricultural volunteers were not sufficiently engaged in nutrition initiatives. People requested more demonstrations and technical support, including for what types of crops can be grown in drought-prone areas.
Interviewer: “After they gave you this seed, were you… taught how to go about the planting?”
Participants: “No.”
Focus group participants, Shangombo District, Zambia
More could be done to scale up programmes that promote the increased production, distribution and affordability of nutritious foods. Making greater progress in this area requires intervening in the political economy of food systems, including building policy dialogues and action plans for improved diets, and stronger engagement between donors, business and governments. Specifically, the Closure Report for HarvestPlus found that further support was needed for the self-sustaining growth of biofortification, including stimulating consumer demand as well as strengthening policies, regulations and the wider enabling environment.
Efforts to improve coordination with partners did not achieve the required level of coverage and convergence of nutrition services on vulnerable households and communities
ICAI found that DFID did not always align with and implement other relevant good practices recommended in the evidence. For several programmes, limited impact was reported to be due to a lack of sufficient population coverage of nutrition services, or the challenge of achieving the convergence of high-intensity nutrition support on the most vulnerable households.
The 2013 Lancet Series recommends that nutrition-specific interventions should be implemented ‘at scale’ to achieve significant reductions in malnutrition. Specifically, ICAI found that DFID and its partners were not always aiming for, or able to achieve, the recommended 90% population coverage. This is primarily due to the large numbers of vulnerable people living in the poorest countries or target regions, for example in the DRC, Nigeria and Bangladesh. In Bangladesh, more than 53 million children make up 32% of the population. According to an evaluation of the nutrition programme we reviewed in the DRC, this was a major constraint on impact. Furthermore, and reflecting a key finding from the 2014 ICAI review, it was not always clear that the full package of recommended nutrition-specific interventions was being delivered by DFID and its partners, or at least to the same level of consistency and quality in a locality (for example due to gaps in health supply chains, the variable capacity of community health workers, or lack of data to evidence take-up). Longer-term, the strategy would be to mainstream the nutrition package within basic health services (as in Ethiopia and Nigeria). However, until then, there is a need for clearer guidance on what constitutes the ‘required package’ of nutrition-specific activities (to have impact) and how the Lancet’s recommended 90% coverage can be achieved, as well as for closer coordination with other donors to pool efforts to maximise coverage.
The lack of a coordinated approach to addressing the multiple determinants of malnutrition has been identified in different sources of evidence as a barrier to achieving nutrition results. It was also a key finding of the 2014 ICAI review, that DFID could do better at implementing programmes in the same places. While nutrition-specific or nutrition-sensitive programmes alone will tackle, if delivered well, some reductions in malnutrition, they will not achieve the maximum possible sustainable reductions in malnutrition without convergence. While DFID aimed to align with evidence that nutrition-specific and nutrition-sensitive programming should converge on the same at-risk populations, by 2019, DFID reported that only 16.8% of its results were ‘high-intensity’. While this partly relates to likely under-reporting of high-intensity intervention (see para 4.14), it also suggests the need for an even greater focus on convergence if reductions in undernutrition are to be achieved.
Figure 12: DFID’s global nutrition results by intensity (2017-18 and 2018-19)
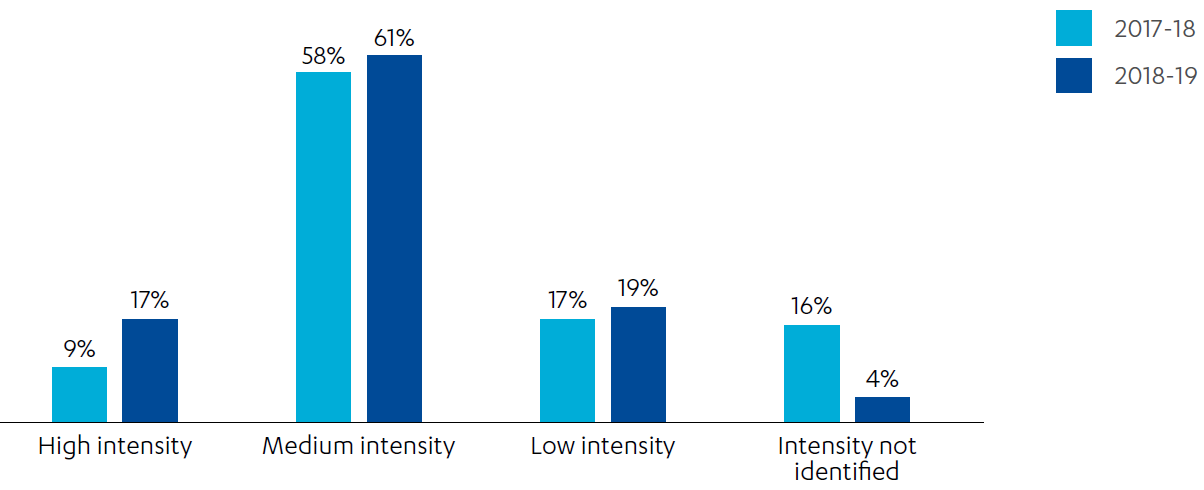
Source: Graphic created from Single Departmental Plan – Results Achieved by Sector in 2015-2018, DFID and Single Departmental Plan – Results Achieved by Sector in 2015-2019, DFID
Achieving convergence is very challenging. Experts highlighted the technical challenge of designing stand-alone nutrition programmes that address multiple causes. Alongside this, ICAI found that there were practical difficulties in ensuring the convergence of different services on vulnerable households, for example in Zambia and Ethiopia. While DFID’s systems strengthening work had made improvements in some areas, obstacles at a local level included the lack of alignment between government expenditure lines, weak or absent coordination structures, and data systems unable to monitor convergence. It should also be noted that there are other public health priorities (for example WASH), and that these may or may not be most urgent in those areas targeted by the portfolio of nutrition programmes. With UK aid’s target countries often facing a variety of priority needs across the population, it can be difficult to concentrate delivery of all required services on specific districts and communities. Despite this, ICAI observed practical examples of the potential for convergence to be realised at the very local level, when donors work closely with government, for example in districts such as Seqota in the Amhara region of Ethiopia. Here, health workers and volunteers were delivering the nutrition-specific health package alongside small-scale agricultural works and training, as part of Ethiopia’s broader social protection programme, backed by government commitments to focus on this area. Local citizens still considered that investments in irrigation and locally grown nutritious foods, alongside safe water and sanitation facilities, needed to be scaled up in order to help reduce undernutrition further.
There are also examples where DFID learnt from these gaps and adapted its approach. The Working to Improve Nutrition in Northern Nigeria programme aims to create stronger links with WASH programming in future, to increase access to water and sanitation facilities in target communities. Zambia’s social protection programme is looking to incorporate ‘cash-plus’ nutrition activities, including behaviour change messaging to encourage the take-up of antenatal services. The second phase of Tackling Maternal and Child Undernutrition in Zambia has introduced additional measures to support convergence: a pyramid approach has been developed that sets out a ‘minimum service package’ across different sectors of support, partners will work together to help achieve 90% coverage of services, and the share of project spend on local service delivery has been increased. During fieldwork in Zambia, effective coordination of services under the new programme was reported by citizens, including joint visits from volunteers to demonstrate how to improve nutritional practices while delivering micronutrient supplementation and treatment for acute malnutrition.
DFID’s advocacy and technical assistance work included efforts to influence and coordinate multi-sector working across different agencies. However, ICAI found that DFID did not always make sufficient efforts to bring other donor and government partners together to ensure that nutrition-specific and nutrition-sensitive programmes converge on the most vulnerable (such as through aligning partner programming). In Ethiopia, it was reported that DFID promoted strong coordination within sectors but could have done more to support cross-sector coordination between donors and government ministries. This is despite important building blocks being in place. ICAI found that the government had developed a system to map the location of donor programmes, but that this was currently underutilised. The government’s Seqota Declaration policy, supported by DFID’s Technical Assistance Programme, identified the nutrition-specific and nutrition-sensitive interventions required to eradicate undernutrition in those wards with the highest burden of stunting. However, the strategy is not fully operational because of funding gaps within the budgets of some line ministries and donors.
Summary
The UK’s nutrition strategy and portfolio have strong potential to be impactful over the longer term, if continued. This is based upon their evidence-based approach, emphasis on strengthening nutrition systems, and positive results. Globally, DFID played a much-valued leadership role with other donors and strategic partners. In 2014, ICAI found that DFID provided valuable technical assistance to build government delivery capacity. Since then, DFID has helped to secure greater government and political ownership and funding commitments to nutrition, despite constrained fiscal contexts. There is a longer-term trend of nutrition improvement in many of countries targeted by DFID, as measured by reductions in stunting.
Global progress on tackling malnutrition is behind schedule and has begun to plateau in recent years. DFID’s programmes have shown a mixed level of impact on undernutrition and were constrained by structural inequalities and recurrent crises. The nutrition portfolio and the work of partners are not yet sufficiently multi-sectoral to address all the underlying drivers of malnutrition and understanding of “what works” in nutrition-sensitive programming can be developed further. While progress has been made in improving the contribution of commercial agriculture programmes, at a country level the portfolio has not sufficiently expanded its focus on working with the private sector and country governments to strengthen nutritious food systems. Achieving sufficiently high population coverage is challenging. The UK and its partners are still to realise the vision of the convergence of services on the most vulnerable communities, as part of fully coordinated country-level strategies for tackling malnutrition.
Conclusion and recommendations
Overall, DFID made important advances following the 2014 ICAI nutrition review. The implementation of nutrition programmes has moved ahead, often as part of longer-term country strategies for tackling undernutrition. DFID exceeded its results target to reach 50 million people (women of childbearing age, adolescent girls and children under five) between 2015 and 2020. The results methodology has now become more sophisticated and has helped to capture and drive an increased focus on quality and multi-sector nutrition delivery, with stronger processes in place to avoid over-reporting. Overall, DFID’s nutrition programmes have been effective, delivering most of their target outputs and (where measured) contributing to outcomes. This has been helped by good partner coordination, successful efforts to foster political leadership of nutrition and DFID’s adaptive approach. The principal weakness of the results methodology and reporting is that they have under-represented the UK’s significant advocacy and technical assistance work globally and in target countries. Given that DFID only started scaling up its work on nutrition in 2013, the positive contributions of UK aid in this area are impressive.
There are challenges in applying complex results methodologies, and the accuracy of programme data needs to be strengthened to improve understanding of coverage, convergence and the inclusion of vulnerable groups. The department’s statistics cadre, as well as improved guidance and common templates, have important roles to play in supporting all staff involved in nutrition interventions, and particularly those at country level, to improve the accuracy of reporting. The UK aid programme needs to work with its partners even more to strengthen national data on the most vulnerable, and to avoid setting up parallel, costly programme systems. As an interim measure, ICAI found strong potential to build on social protection systems and their data on vulnerable households.
DFID’s nutrition programmes have been well targeted towards countries, areas within countries and population groups most vulnerable to undernutrition. Although DFID often worked in very challenging environments, with climate and conflict-related crises limiting access to and heightening the vulnerability of women and children, the department managed to reach its target groups. This was achieved through a combination of strengthening local coordination structures, working within the existing health system, and outreach approaches involving community health workers and volunteers from different sectors. Based upon ICAI’s 2014 recommendations, we might have hoped to see more progress on the inter-related areas of targeting the most vulnerable mothers and children, and strengthening national and programme data systems. However, we recognise the challenges of combining this with achieving high coverage and ensuring government ownership. The new department could do more to understand and reach the most marginalised within its target groups. DFID’s technical assistance support was not sufficiently focused on filling this gap, and FCDO could strengthen citizen consultation mechanisms to help amplify the voices of the most vulnerable.
DFID’s nutrition programming was well aligned with evidence of “what works”, including combining nutrition-specific support with the scaling up of nutrition-sensitive interventions. Alongside this, the department continued to make contributions to mobilising the global community, and further strengthened the capacity of overseas governments, their commitments, and action on nutrition, since 2014, to help meet the global nutrition goals. Because of these factors, and evidence of broadly positive interim results, ICAI concludes that the UK aid programme’s nutrition portfolio is likely to impact positively on undernutrition over the longer term, if continued. Although it is difficult to attribute directly to DFID’s programmes, most countries within our sample have seen reductions in stunting.
More recently, progress in reducing undernutrition is beginning to plateau. This is due to underlying structural inequalities and recurrent climate and conflict shocks, compounded by frontline delivery constraints within underfunded health care systems that limit the coverage of services. ICAI found that the nutrition work of UK aid (and its partners) needs to be embedded more comprehensively across sectors, to help tackle these constraints. In particular, there is a need for a stronger focus on strengthening nutritious food systems, including through agriculture programmes and technical assistance to governments. The 2014 ICAI review recommended that DFID explore how to engage the private sector in nutrition, and they had begun to do this, but there is a need to scale up this work. More generally, relevant and impactful nutrition-sensitive programming (and associated performance metrics) could be developed to help provide the nutrition boost across the wider aid portfolio. There needs to be more focus on the convergence of nutrition-specific and nutrition-sensitive programmes (including agriculture and WASH), through improved coordination across government, and other partners as well as donors. Overall, for the UK to achieve its goals of reducing undernutrition, the aid programme needs to work up more coherent strategies for tackling nutrition at country level, supported by increased funding commitments from relevant line ministries.
Although this report looks back at DFID’s work, our recommendations are directed to the FCDO following the merger of DFID with the Foreign and Commonwealth Office, and are intended to strengthen the new department’s future approach to nutrition. Sustaining efforts to eradicate malnutrition is critical to the UK’s Ending Preventable Deaths strategy, resilience to pandemics and other crises, and wider development goals. Continued prioritisation of nutrition investments and systems building is needed to capitalise on the positive progress made to date.
Recommendations
Recommendation 1:
FCDO should capture and communicate progress against all goals in its nutrition strategy, including strengthening systems and leadership for improved nutrition.
Problem statements:
- DFID’s nutrition reporting has focused on programme reach, while its nutrition strategy has incorporated more commitments including fostering nutrition leadership, building national capacity, and leverage of the private sector.
- The lynchpin Technical Assistance for Nutrition programme has not been systematically assessing and reporting on its impact on nutrition leadership, financing, and coverage of services.
- DFID’s advocacy and technical assistance and innovative nutrition-sensitive programming have not been fully visible, limiting the potential for learning internally and externally.
Recommendation 2:
FCDO should strengthen statistical capacity and quality assurance in-country and centrally, to support more accurate measurement of programme coverage and convergence, and to use the data to improve nutrition programming.
Problem statements:
- Factors such as the poor quality of monitoring systems and gaps in statistical capacity in DFID country offices have made it more challenging to provide accurate measurements of reach.
- DFID has not had a common template for country offices to capture and aggregate their nutrition results.
- There has been no detailed guidance in DFID’s methodology note, nor a systematic sharing of good practices across country offices, to support more accurate measurement of coverage and convergence (including accounting for partner contributions).
- Results data has not been consistently used to guide programme design and drive greater convergence, or to inform advocacy and systems building work.
- Not all country offices have been producing the recommended narrative report to support lesson learning.
Recommendation 3:
FCDO should strengthen systems for identifying and reaching the most marginalised women and children within its target groups.
Problem statements:
- There has been a lack of analysis of which groups of women and children are most at risk of undernutrition.
- A lack of disaggregated targets and limited data has meant that DFID has not been consistently identifying and reaching the most acutely vulnerable households.
- There has been a lack of systematic guidance on how to engage with the hardest-to-reach groups.
- Existing poverty targeting mechanisms developed through DFID’s social protection programmes have not been fully exploited to help identify and reach the most acutely vulnerable households.
- DFID has been heavily reliant on community workers to identify and reach the most vulnerable, which is not always effective, particularly during crisis situations.
Recommendation 4:
FCDO should more consistently gather citizen feedback to help improve and tailor its nutrition programmes.
Problem statements:
- Nutrition programme design and delivery have not always been informed by the voices of citizens.
- Opportunities have been missed to tailor nutrition programmes better, and target them more effectively.
- DFID has made insufficient efforts to understand the needs of the most vulnerable groups and what the underlying causes of their vulnerability are.
Recommendation 5:
FCDO should scale up its work on making sustainable and nutritious diets accessible to all, to help address the double burden of malnutrition, through nutrition-sensitive agriculture and private sector development.
Problem statements:
- Due to gaps in the multi-sector approach of DFID and its partners, some underlying drivers of undernutrition, such as lack of access to nutritious diets and access to WASH facilities, have been insufficiently addressed.
- Coordinated work across country governments, donors, small and medium-sized enterprises, and other partners on strengthening the increased production, distribution and affordability of nutritious foods has been weak.
- There has been a lack of detailed guidance from DFID on effective nutrition-sensitive programming in climate-smart agriculture and other sectors, and on what relevant outcomes should be measured.
Recommendation 6:
FCDO should work more closely with its partners to achieve the convergence of nutrition interventions, by aligning different sector programmes to focus on those communities most vulnerable to malnutrition.
Problem statements:
- National nutrition coordination platforms, involving DFID, other donors, and governments, have not been sufficiently focused on converging nutrition interventions on the most vulnerable communities.
- DFID and its partners have not always achieved 90% population coverage in target areas.
- There has been a lack of detailed programme mapping undertaken to help plan convergence.
- There has been a lack of funding commitments and accountability across key sectors.
- There has been a lack of sub-national capacity for coordination and delivery.
Annexes
Annex 1: List of countries and programmes in the sample