CDC’s investments in low-income and fragile states
Score summary
CDC has made progress in redirecting investments to low-income and fragile states, but has been slow in building in-country capacity to support a more developmental approach. CDC has not done enough to ensure or monitor development results, or to progress plans to improve evaluation and apply learning.
The CDC Group plc (CDC) is the UK’s development finance institution (DFI), wholly owned by the Department for International Development (DFID). Over the period of this review, from 2012 to 2018, CDC has played an increasing role in DFID’s economic development strategy. DFID has set CDC progressively more ambitious goals for achieving development impact in low-income and fragile states, and has reduced its financial return targets to facilitate this. DFID invested £1.8 billion of new capital into CDC over the four-year period from 2015 to 2018, with further injections planned through to 2021. This shift in strategy has required a fundamental transformation in the leadership and culture of CDC, a significantly expanded workforce with new skills, and major changes to products and practices.
CDC has made significant progress with this transformation, with more changes planned. It has successfully redirected new investments towards lower-income and fragile states and its priority sectors, though these are largely concentrated in a few countries and in the infrastructure and financial services sectors. It has diversified its investment products to include direct equity and debt; piloted innovative financial instruments and introduced a new ‘Catalyst Portfolio’ that invests in riskier markets; and it has increased its focus on development impact.
We welcome these changes, but note that a number of important activities have only recently been launched and it is therefore too early to assess their effectiveness or ultimate impact. Earlier progress on deployments to country offices, particularly in Africa, on the development of geographic and sectoral plans, and on monitoring and evaluation would have helped to accelerate the scale-up of investment and the achievement of broader development impact in these more challenging markets.
For most of the review period, CDC’s lack of clarity on expected development impact, its monitoring of a narrow set of impact metrics and the absence of comprehensive, independent evaluation made it difficult for us to assess its overall impact. From 2018, CDC began to significantly enhance its processes for impact management, monitoring and evaluation. However, there is more still to do to encourage impact, from the selection of investments through to portfolio management and exits. CDC’s leadership among DFIs in assessing and supporting the environmental, social and governance issues of its investees provides an indication of what could be achieved on impact more generally.
CDC has increased its resources for learning throughout the review period. There are examples of thoughtful and strategic research in priority areas, but these do not yet add up to a learning effort commensurate with the scale of CDC’s investment. We found that CDC has not maximised learning on development impact from its own investments, and that there is limited evidence of CDC gathering and applying learning on working in the most difficult investment markets.
| Individual question scores | |
|---|---|
| Question 1 Relevance: Does CDC have a credible approach to achieving development impact and financial returns in low-income and fragile states? |  |
| Question 2 Effectiveness: How effective are CDC's investments in low-income and fragile states? |  |
| Question 3 Learning: How well does CDC learn and innovate? | |
Executive summary
CDC is the UK government’s development finance institution (DFI), wholly owned by the Department for International Development (DFID). Its mission is to promote economic development by investing in businesses in developing countries where markets are weak and where access to private finance is limited and expensive. As an aid-spending body, CDC aims to achieve a positive development impact. As a DFI, it is also expected to generate a financial return on its investment portfolio, which is recycled into future investments.
CDC’s importance within the UK’s aid portfolio has grown substantially. Between 2015 and 2018, it received investments of new capital from DFID totalling £1.8 billion. Further injections are planned through to 2021, with CDC projecting that its net assets may increase from £2.8 billion in 2012 to over £8 billion by 2021.
CDC plays a key role in DFID’s economic development strategy, which emphasises the reduction of poverty through building markets and trading ties, and catalysing private investment to create jobs and services. Aside from improving the investment climate and promoting economic growth, CDC also aims to contribute to poverty reduction through investments that improve access to essential goods and services for the poor.
Under a new investment strategy agreed with DFID in 2012, CDC shifted its investment focus towards lower-income and fragile states in Africa and South Asia, including challenging markets where investments are riskier and harder to find. This has required a fundamental transformation in the leadership, management and culture of CDC, a significantly expanded workforce with new skills and experience, and major changes to the organisation’s products and practices.
This performance review focuses on how well CDC has adapted its strategy, portfolio and organisational capacity to meet the challenge of achieving development impact in low-income and fragile states. It covers the period from 2012 to 2018.
Relevance: Does CDC have a credible approach to achieving development impact and financial returns in low-income and fragile states?
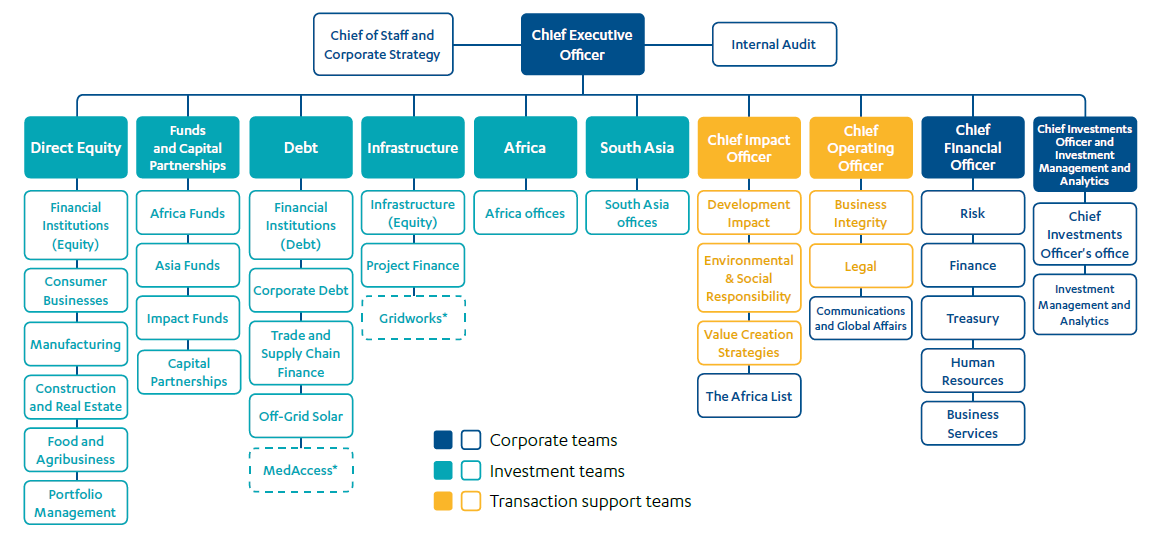
Since 2012, CDC has increased its emphasis on development impact and shifted its focus towards investing exclusively in low-income and fragile countries. In 2013, it began to use a Development Impact Grid, developed jointly with DFID, to screen potential investments and direct capital towards geographies and sectors with greater potential for development impact. The grid scores prospective investments along two axes: the investment difficulty of the country (or Indian state) and the potential of the sector to create jobs.
Between 2004 and 2012, CDC only invested indirectly, through intermediary funds. Since 2012, it has diversified its range of investment products to include direct equity and direct debt, has piloted innovative new financial instruments and is now expanding its technical assistance grants to give it more flexibility to support businesses in challenging investment environments.
In 2017, CDC created a separate ‘Catalyst Portfolio’ to facilitate higher-risk investments with the potential for greater development impact in poorer communities and places. This has a lower ‘profitability hurdle’ (or target financial return) than its main portfolio, now called the ‘Growth Portfolio’. CDC has not set a firm target for the size of its Catalyst Portfolio but does not expect it to account for more than 20% of total investment by CDC.
CDC’s most recent corporate strategy, its 2017-21 strategic framework, includes commitments for new sector strategies, a larger in-country presence and enhanced monitoring and evaluation. CDC also aims to expand its knowledge of how to achieve development impact, including in areas such as women’s economic empowerment, and to develop new investment instruments to increase its reach in the most difficult markets. While we welcome these commitments, we conclude that CDC could have done more at an earlier stage in each of these areas. It is too early to determine how significant these changes will be in shaping future investment decisions or improving impact.
CDC collaborates well with DFID centrally, but the relationship is not as developed at country level, so there is a risk that opportunities for collaboration and knowledge sharing between CDC and DFID are being missed. We saw some positive examples of joint working on our country visits, but these were mainly one-off activities.
CDC re-established a country presence in India in 2013 but has been slow to establish offices elsewhere. At the end of 2017, it had ten staff in India but only seven in all of Africa, out of the total CDC staff of 266. A stronger country presence would help with sourcing investments, impact management and monitoring and evaluation. It would also facilitate coordination with DFID and with other development partners. CDC plans to open four regional offices in Africa by 2019, with single representatives in three further countries.
CDC identified seven priority sectors at the start of the review period but did not begin preparing comprehensive sector strategies until 2018. It does not have geographic strategies and instead plans to develop ‘country perspectives’ in the coming years that will collate existing information on economic development priorities and the private sector.
In summary, CDC has made important progress since 2012 in reorienting its strategy and plans, and transforming the organisation, to meet the very significant challenge of achieving both development impact and financial returns in more challenging markets. We have therefore awarded a green-amber score for relevance. However, the transition is not yet complete and many important initiatives are at an early stage. Given the commitment to additional capital injections by DFID, CDC needs to make further rapid progress in building staff capacity, strengthening its country network and developing and implementing its new strategies and plans for achieving development impact.
Effectiveness: How effective are CDC’s investments in low-income and fragile states?
CDC has made progress in redirecting its capital towards priority sectors in lower-income and fragile countries. Between 2012 and 2017, 52% of the investments made in the Growth Portfolio were in countries classified as difficult investment environments (up from 23% in 2009-11). However, most of these investments were concentrated in a few of the larger economies in this category (such as Kenya and Nigeria) and most of its investee companies were headquartered in the more prosperous areas of these countries, particularly the capitals.
For most of the review period, CDC relied mainly on the Development Impact Grid to screen investments for their potential benefit to poor people, focusing on job creation potential. While it was a useful innovation, the grid is a relatively blunt instrument for assessing potential development impact, with a narrow focus on jobs. We believe that CDC should have done more to select impactful investments.
Beyond the decision to invest, CDC did not set targets or expectations for development impact, nor did it do enough to encourage opportunities to enhance development impact. Until recently, it also monitored only a narrow set of metrics, making it difficult to assess CDC’s overall impact, both at the investment level and for the portfolio as a whole, for much of the review period.
From 2018, CDC has introduced improvements to the assessment and monitoring of impact, supported by new ‘development impact cases’ for all potential investments and a significantly expanded team of development impact experts. We welcome these developments, which have the potential to broaden CDC’s impact and strengthen its approach to tracking progress. CDC needs to embed these new processes and resources quickly and systematically into investment sourcing, screening and management across its product teams, to support its ambitions for development impact.
CDC is a leader among DFIs in assessing and supporting environmental, social and governance (ESG) issues. Its success in helping and encouraging funds and investees to improve their practices in these areas provides an indication of what could be achieved in relation to development impact more generally.
We recognise the scale of the challenge that CDC faces in delivering impact in more difficult markets while simultaneously expanding its portfolio, and the considerable progress that has been made. However, we also note that DFID has given CDC more room to pursue development impact by reducing its financial return targets to just 3.5% for its Growth Portfolio, and ‘at least break even’ overall. Yet in the six years to December 2017, CDC’s average financial returns across the portfolio were 10.6%. CDC forecasts lower returns in the coming period, due to a more challenging investment climate and because of the increasing focus on delivering impact in difficult markets. The figures nonetheless suggest that CDC could have pushed harder on achieving development impact, while still meeting its financial return hurdle.
We are encouraged by the increased emphasis on development impact, both at the investment selection stage, where DFIs have the greatest opportunity to maximise their impact, and through deploying additional resources and expertise to support the assessment and management of impact. However, we believe that these improvements could have been made earlier, and that CDC did not do enough to maximise the impact of its investments for most of the review period. We have therefore given CDC an amber-red score for the effectiveness of its $1.5 billion of new investment in low-income and fragile states between the start of 2012 and end of 2017.
Learning: How well does CDC learn and innovate?
Despite recent improvements, CDC’s learning efforts are not yet sufficiently adapted to its ambition to deliver development impact at scale in low-income and fragile states.
CDC commissioned a small number of thoughtful and strategic research projects during the review period. However, more could have been done earlier, particularly to support its priority sectors. The impressive health impact framework, published in 2017, provides an example of what could be achieved across these sectors.
Before 2017, CDC had no strategic plan for using monitoring and evaluation results to inform its investment choices and made limited attempts to investigate the development impact of investments through evaluation studies. It also did not do enough to capture learning systematically from across its investments in the most difficult markets. CDC has recently adopted new plans for strengthening its evaluation and learning practices. However, important sector-wide evaluation studies have yet to be commissioned, two years into the new strategy.
CDC has recently increased its focus on sharing learning. It has created new staff roles and revamped its website in order to help share learning, building upon an existing programme of seminars and speaker events. However, we saw only a few examples of learning on development impact informing CDC’s investment decisions and portfolio management practices. Embedding evaluation and learning as part of core working practices within CDC’s investment teams represents an ongoing challenge.
CDC is recognised as a thought leader by other DFIs in some areas, particularly on ESG issues. However, CDC could learn more from other DFIs and from relevant civil society organisations. More could also be done to share learning between CDC and DFID, in particular in relation to sector priorities and at the country level.
We have awarded CDC an amber-red score for learning, reflecting the weaknesses and gaps in evaluation and learning for most of the review period. We welcome the commitment to scaling up evaluation efforts and the production of sector-specific learning products, but believe that CDC needs to embed a stronger culture of learning across the organisation.
Conclusions and recommendations
CDC has made progress in redirecting investment to low-income and fragile states, but has not done enough to secure or monitor development gains, to improve evaluation or to apply learning. It is implementing ambitious plans to address these concerns, but these are mostly at an early stage. We have therefore awarded CDC an amber-red score overall.
We offer a number of recommendations to help CDC increase its development impact in low-income and fragile states:
Recommendation 1
CDC should incorporate a broader range of development impact criteria and indicators into its assessment of investment opportunities and ensure these are systematically considered in the selection process.
Recommendation 2
CDC should take a more active role in the management of its investments, using the various channels available to it to promote development impact during their lifetime.
Recommendation 3
CDC should strengthen the monitoring and evaluation of the development impact of its investments and the learning from this, working with DFID to accelerate their joint evaluation and learning programme.
Recommendation 4
CDC should work more closely and systematically with DFID and other development partners to inform its geographic and sectoral priorities and build synergies with other UK aid programmes to optimise the value of official development assistance.
Recommendation 5
In the presentation of its strategy and reporting to stakeholders, CDC should communicate better its approach to balancing financial risk with development impact opportunity, and the justification for its different investment strategies.
Recommendation 6
DFID’s business cases for future capital commitments to CDC should be based on stronger evidence of achieved development impact and clear progress on expanding their in-country presence.
Introduction
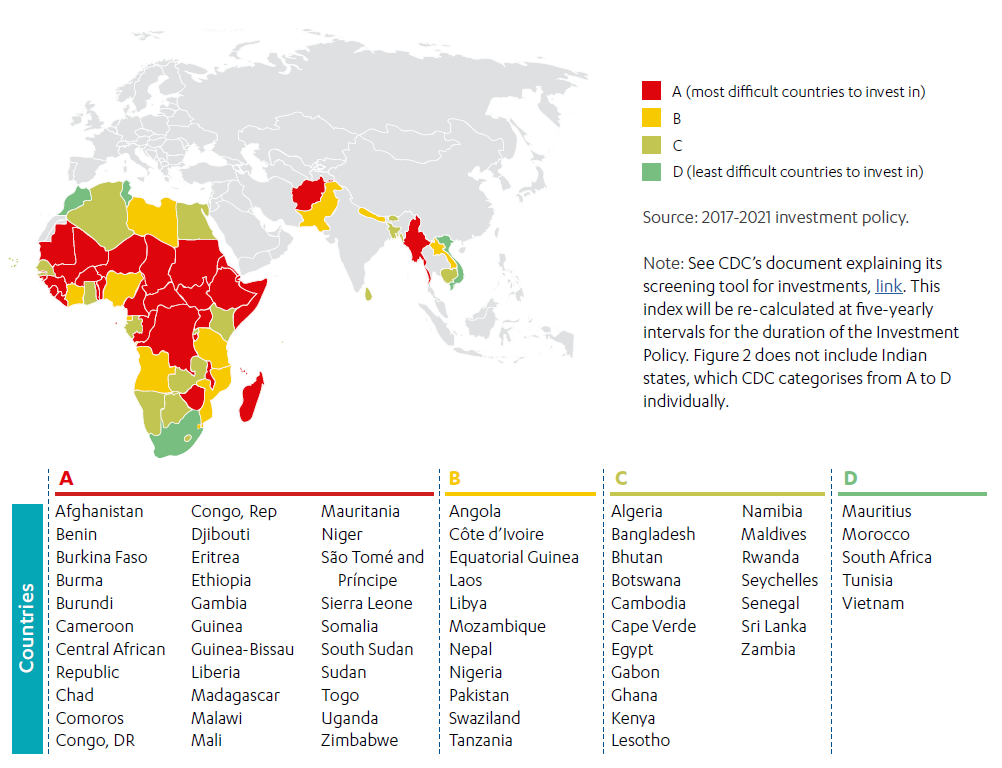
CDC Group plc is the UK’s development finance institution (DFI), wholly owned by the Department for International Development (DFID). It is the oldest DFI in the world: since its creation in 1948, it has invested in thousands of businesses in emerging markets and developing countries. Its mission today is “to support the building of businesses throughout Africa and South Asia, to create jobs and make a lasting difference to people’s lives in some of the world’s poorest places”. It is expected to generate a financial return on its investments which is then reinvested, enabling its portfolio to grow over time.
Between 2004 and 2012 CDC invested mainly through intermediary funds, and between 2004 and 2009 it focused predominantly on middle-income countries such as India and South Africa. In 2010, the then secretary of state for International Development, Andrew Mitchell, announced plans to “reconfigure” CDC to align it better with DFID’s strategic priorities. He stated, “I want CDC to be more pro-poor focused than any other Development Finance Institution, doing the hardest things in the hardest places.”
This transformation began in earnest in 2012. CDC shifted its investment focus towards lower-income and fragile states in Africa and South Asia and into sectors with the greatest propensity to create jobs. It diversified into new investment products, piloted innovative financial instruments and, in 2017, introduced a separate portfolio, the ‘Catalyst Portfolio’, to support transformational change in difficult markets.
In its 2012-16 strategy, CDC’s primary focus was on delivering development impact through job creation. In 2017, CDC broadened its ambitions for development impact, for example to include support for a range of Sustainable Development Goals and women’s economic empowerment.
This shift in strategy and focus has involved wholesale organisational change at CDC, with a largely new management team, major changes in culture, systems and processes and significant recruitment – the workforce increased from just 47 in 2012 to 308 by mid-2018.
CDC has become an increasingly important channel for UK aid. Between 2015 and 2018, CDC received investments of new capital from DFID totalling £1.8 billion, and further capital injections of up to £703 million per annum are planned until 2021. CDC’s net assets are projected to increase from £2.8 billion in 2012 to above £8 billion by 2021 as a result of these capital injections and earnings.
This review covers the period from 2012 to 2018. During this time, DFID has become a more active and engaged shareholder in CDC. However, CDC remains a separate corporate entity. In particular, individual investment decisions by CDC are made independently of DFID.
Seven years on from the start of this transformation, this is an appropriate time to review the progress that CDC has made in refocusing its efforts towards promoting economic growth in low-income and fragile states. As CDC is a long-established DFI and because of the scale of new investment by DFID, we have conducted a performance review (see Box 1 for ICAI’s review types).
Box 1: What is an ICAI performance review?
ICAI performance reviews take a rigorous look at the efficiency and effectiveness of UK aid delivery, with a strong focus on accountability. They also examine core business processes and explore whether systems, capacities and practices are robust enough to deliver effective assistance with good value for money.
Other types of ICAI reviews include impact reviews, which examine results claims made for UK aid to assess their credibility and their significance for the intended beneficiaries, learning reviews, which explore how knowledge is generated on new or recent challenges for the UK aid programme and translated into credible programming, and rapid reviews, which are short, real-time reviews examining an emerging issue or area of UK aid spending.
The review explores how well CDC has reoriented its investment approach and portfolio to achieve development impact in low-income and fragile states, while still delivering its intended financial return. The review questions we have answered are set out in Table 1.
Table 1: Our review questions
| Review criteria and questions | Sub-questions |
|---|---|
| 1. Relevance: Does CDC have a credible approach to achieving development impact and financial returns in low-income and fragile states? | • What progress has CDC made towards establishing an appropriate and coherent strategy for achieving development impact at scale in low-income and fragile states? • How well has CDC adapted its ways of working to invest in more challenging markets while managing a rapidly growing portfolio? |
| 2. Effectiveness: How effective are CDC’s investments in low-income and fragile states? | • How well does CDC select, manage and exit investments in lowincome and fragile states? • How effectively does CDC maximise its development impact while meeting financial return targets? • How well does CDC add value to individual companies, support their inclusive and sustainable growth and meet responsible investment commitments? • How effectively does CDC contribute to establishing and expanding investment markets in low-income and fragile contexts? |
| 3. Learning: How well does CDC learn and innovate? | • How well has CDC learned from global evidence on impact investment in difficult markets? • How well do CDC’s monitoring and evaluation processes drive learning within the organisation? • How well is CDC sharing learning (in support of a leadership role within the investment industry)? |
The review builds on previous parliamentary and National Audit Office (NAO) reviews of CDC (see Box 5). The 2016 NAO review focused on DFID’s oversight of CDC and CDC’s approach to managing its business. Our primary focus is on CDC’s ability to deliver results in low-income and fragile states.
Box 2: How this report relates to the Sustainable Development Goals
The Sustainable Development Goals (SDGs), otherwise known as the Global Goals, are a universal call to action to end poverty, protect the planet and ensure that all people enjoy peace and prosperity. CDC’s investment in opportunities in developing and emerging markets can play an important role in achieving a number of SDGs.
Related to this review:
 Goal 8: promote sustained, inclusive and sustainable economic growth, full and productive employment and decent work for all
Goal 8: promote sustained, inclusive and sustainable economic growth, full and productive employment and decent work for all
CDC prioritises job creation because it gives people the income, opportunity and dignity to live better lives. It aims to do this through supporting economic development and by growing businesses in developing markets where few large employers currently exist. Successful and well-managed investments could lead to significant and sustainable job creation in these markets.
 Goal 1: end poverty in all its forms everywhere
Goal 1: end poverty in all its forms everywhere
CDC aims to tackle poverty through supporting businesses and through growing investment markets, thus contributing to economic growth, job creation, increased tax revenues and enhanced access to basic services.
In addition, CDC supports firms providing goods and services that are aligned with a number of other sectoral SDGs – for example SDG 3 (health), SDG 4 (education), SDG 7 (energy), SDG 9 (infrastructure, industrialisation and innovation) and SDG 13 (climate change). Due to the range of its investments, CDC’s work spans almost all the SDGs.
Methodology
The review covers the period from 2012 to 2018. It explores the reconfiguring of CDC and its strategy, approach and portfolio towards investment in low-income and fragile states.
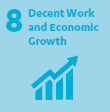
Our methodology included four components (see Figure 1), as follows:
- Literature review: We reviewed the literature on development finance institutions (DFIs), including academic literature and publications by bilateral and multilateral development institutions. This informed our understanding of current debates on impact investment by DFIs and the challenges of investing effectively in low-income and fragile states. We drew lessons from the literature on ‘what works’ in areas such as promoting development impact and on best practice in monitoring and evaluation.
- Corporate review: We assessed the effectiveness of CDC’s processes for identifying investments and measuring their development impact, and of its evaluation and learning processes, up to the end of 2018. We mapped how CDC has adapted its staffing, resource allocation and ways of working to build its capacity to work in more difficult markets and maximise its development impact. This included a review of CDC’s corporate-level documentation and management information, including relevant policies, frameworks and operational plans, and interviews with key stakeholders within CDC and DFID. We also engaged with a wide range of external stakeholders, including academics, experts and representatives of other DFIs.
- Investment team reviews: Investment teams are the internal structures through which CDC identifies, assesses, executes and monitors investments, dealing with different product types, sectors or regions. We selected six out of CDC’s 12 investment teams and sampled 19 investments made by these teams between 2012 and 2017, to explore how CDC operationalises its approach to achieving development impact and financial returns in more difficult markets (see our sampling criteria and approach below, and further details in Annex 1). We also examined 12 potential investments that were ultimately not made. For each of the investment teams in our sample, we reviewed documentation and evidence, and interviewed relevant staff, investees and other stakeholders, in relation to the decisions to invest and the subsequent management of the investments. Where the investment was in a fund, we reviewed the documentation in relation to that investment at a portfolio level, but also reviewed an additional sample of investments made by that fund. For all sampled investments, we reviewed their development impact and the quality of CDC’s assessments of potential and achieved development impact.
- Country visits: We visited Kenya, Malawi, Nigeria and Tanzania to assess a sample of investments in each country. We interviewed CDC and investee staff, as well as other in-country stakeholders, such as DFID economic advisers and external sector experts, and explored the relevance of CDC’s investment approach to the country context, and the plausibility and significance of its reported development impact.
Figure 1: Overview of the methodology
Both our approach and this report have been independently peer- reviewed.
Sampling criteria and approach
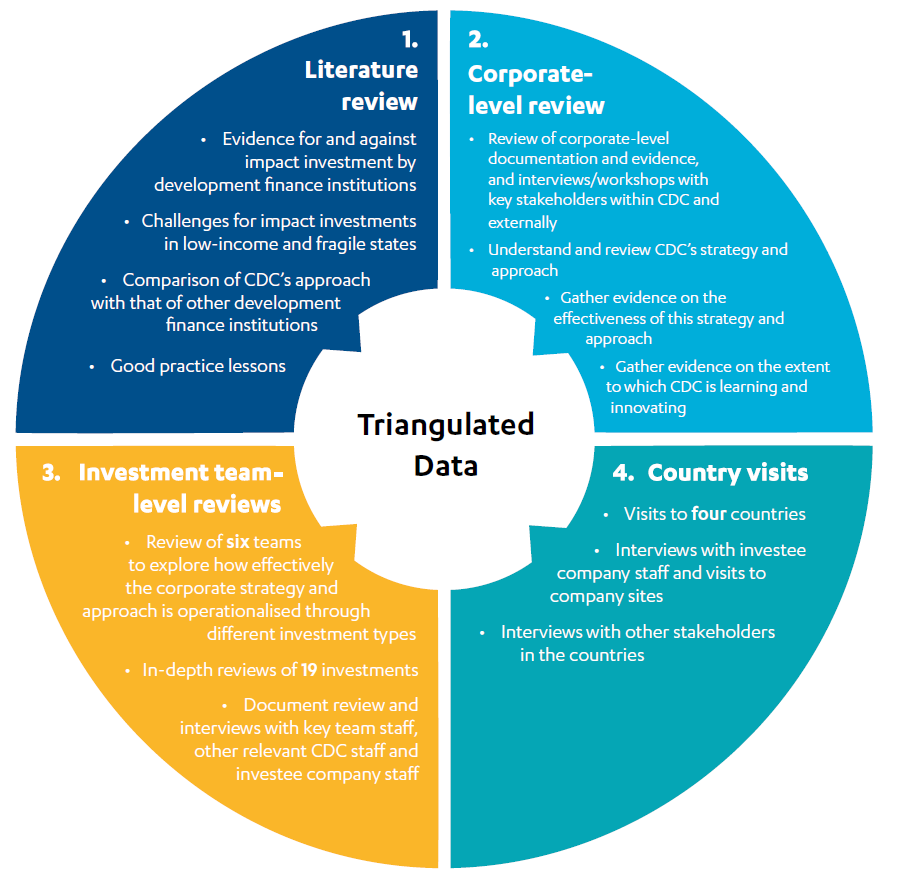
The review focuses on CDC’s progress in building its portfolio in low-income and fragile states. We used CDC’s own categorisation to identify its most difficult investment locations and selected only countries that over the period were classified as A and B – the two most difficult investment categories (see Figure 2).
We selected six out of CDC’s 12 investment teams (based on CDC’s internal organisation structure as of the start of 2018). We then selected a small, random sample of investments by these teams within the two most difficult investment categories, as well as a small sample of rejected deals, for in-depth review. (For more information on the sample of investments, see Annex 1.) The six teams were chosen based on the significance of their investment in difficult markets, their use of both direct and indirect investments, and their ‘market building’ strategies – this last factor being particularly relevant in low-income and fragile countries.
The majority of our sample was drawn from investments made between 2012 and 2016, to allow a sufficient period after the investment was made to be able to assess likely impact. However, it included a small number of fund and Impact Accelerator transactions through to December 2017.
Figure 2: CDC’s categorisation of countries in which it invests in by investment difficulty
Box 3: Limitations to the methodology
Some of the changes to CDC’s resourcing, systems and processes were only set in motion with its new strategic framework in 2017. It is therefore premature to assess the effectiveness of these new developments. In these circumstances, we have focused on likely effectiveness, based on analysis of the strategies and approaches being pursued and early evidence of performance, triangulated through interviews with expert stakeholders.
We reviewed a sample of 19 out of 345 new investments made between 2012 and 2017. This sample is not representative of CDC’s portfolio or of its investments in more challenging markets. However, these investment reviews, complemented by our review of CDC’s investment strategies and processes, enabled us to make informed judgments about CDC’s approach to investing in low-income and fragile states. We did not review any new investments made in 2018 because it was too early to assess their impact or effectiveness, although we reviewed the processes involved in their selection.
Some of the information that CDC holds on its investee companies is commercially sensitive. In writing this report, we have respected CDC’s obligation to keep this information confidential. This has not restricted our ability to make informed judgments.
Background
The rise of development finance institutions
Since the early 2000s, donors have made more use of development finance institutions (DFIs) to promote private sector development and economic growth in developing countries. Between 2002 and 2014, new investments by DFIs grew from $10 billion to around $70 billion per year – an increase of 600%. This is equivalent to half the value of all annual global official development assistance (ODA). An important part of the rationale for DFIs is that they can successfully demonstrate the viability of investment in developing country markets that are neglected by private investors and the financial markets – thereby helping to mobilise or ‘leverage’ larger flows of private finance. They therefore have a key role in the ‘billions to trillions’ agenda, which recognises that the Sustainable Development Goals will require a huge increase in funding from many sources, not just ODA.
DFIs deploy development capital through loans, equity investments, guarantees and other investment instruments to generate development impact and financial returns. They may also provide grants and non-financial support. The main types of investment instruments used by CDC are set out in Box 4.
Box 4: Main investment instruments used by CDC
Debt: CDC provides loans to businesses and projects in its priority sectors in four ways: project finance (with tenors of up to 18 years), corporate finance, trade finance and loans to financial institutions.
Direct equity: CDC provides capital funding to investee companies by purchasing shares (‘equity’) in companies. Where it is a significant shareholder, CDC generally has a position on the company’s board of directors and so is able to influence the strategy and operations of the investee.
Intermediated equity: CDC continues to invest via funds that invest in a range of companies, helping to develop local investment capacity and mobilise capital from commercial investors. The funds are able to invest in more and smaller businesses than CDC is able to directly.
Through their investments, DFIs aim to contribute to a range of development impacts. Their objectives include creating jobs, expanding the provision of goods and services, increasing tax receipts for developing country governments, building investment markets and improving the management practices of investee firms and funds. It is widely believed that, by contributing to private sector development, DFIs promote economic development and poverty reduction.
However, there is a relative lack of rigorous evidence of DFIs’ impact on poverty. This is due in part to methodological challenges in establishing the links between a portfolio of investments and wider development outcomes, but also to gaps and weaknesses in monitoring and evaluation. For example, in 2011, the World Bank’s Independent Evaluation Group concluded that fewer than half of the investments made by the World Bank’s DFI, the International Finance Corporation, were accompanied by the systematic collection of evidence on their impact on poverty reduction.10 Historically, some DFIs have also been criticised for focusing too much on middle-income countries such as India, where investment opportunities are relatively plentiful.
Box 5: Previous scrutiny of CDC and its development impact
In the past decade, a number of scrutiny bodies have undertaken assessments of CDC and its development results:
- In 2008, the National Audit Office (NAO) published a report on DFID’s oversight of CDC. It concluded that CDC had “made a credible contribution to economic development” while also encouraging the engagement of other foreign investors. However, it highlighted the challenges that CDC faced in converting its pipeline of potential deals into investments, raised questions about its additionality, and noted that further evidence was needed on whether CDC’s investments were an effective way of providing direct or indirect economic benefits for the poor.
- A report by the Public Accounts Committee, which built on the NAO report together with an evidence session with senior officials from DFID and CDC, also found that there was limited evidence of CDC’s effects on poverty reduction, as well as emphasising the need to invest more in low-income countries.
- In 2011, the International Development Committee published a report on the future of CDC. It raised concerns as to whether CDC was delivering sufficient development impact. In particular, it questioned whether some of its investments duplicated those that would have been made anyway by private investors, potentially distorting rather than building investment markets. It also found that over half of its investments were in middle-income countries, and too few in sectors that most benefit the poor.
- In 2016, the NAO conducted another review of CDC. It found that CDC had made progress in aligning its portfolio with DFID’s priorities, but that more evidence was needed on its development impact. It criticised DFID for not doing enough to evaluate its impact.
- This was followed by another report from the Public Accounts Committee, which commented on DFID’s failure to seek independent advice before its 2015 capital injection in CDC and the lack of targets reflecting the varied nature of CDC’s portfolio. It also noted the difficulty of reaching firm conclusions about CDC’s development impact.
The increasing focus on economic development, the private sector and CDC in the UK’s aid strategy
The growing importance of development capital and leveraging private sector investment to address global challenges has been reflected in developments in UK aid. DFID has rebalanced its portfolio towards the promotion of economic development, with an increasing emphasis on growth and job creation as engines of poverty reduction. DFID’s Structural Reform Plan in 2010 announced wealth creation as one of its main priorities. In 2011, DFID’s new Private Sector Development Strategy stated that it would engage with firms, directly and indirectly, to help them generate jobs, opportunities, income and services for poor people. Promoting global prosperity is also one of the strategic priorities of the UK’s 2015 aid strategy, while new economic development strategies in 2014 and 2017 set out DFID’s priorities on economic development, including affirming CDC as a major partner in this work.
CDC’s 2011 Business Plan and 2012-16 Investment Policy, formulated and issued jointly with DFID, signalled important changes to CDC’s strategy, with the intention of increasing its development impact. This heralded a major transformation in CDC’s organisation and investment activities.
Figure 3: The history of CDC
From 2012, CDC shifted its investment focus away from middle-income countries and towards lower-income and fragile states in Africa and South Asia, in sectors that create the most jobs. It also diversified into new investment products, investing directly as well as through funds, and piloted innovative financial instruments. In 2017, it introduced a separate ‘Catalyst Portfolio’ to support transformational change in difficult markets.
New product teams were established to manage direct investments, and a new Development Impact team was formed. Most recently, CDC set up a value creation strategies team to focus on its commitments in the areas of skills and leadership, job quality, gender equality and climate change, working alongside the established environmental and social responsibility (E&S) team. The E&S team ensures that companies meet minimum environmental and social standards, as well as supporting those with the potential to improve their practices through what CDC terms its ‘value additionality’ offering.
These changes involved major adjustments in the leadership and management of CDC, a considerably expanded workforce and wholesale changes in the culture, systems and practices of the organisation.
Figure 4: Evolution of staffing of CDC’s teams relevant to the investment process
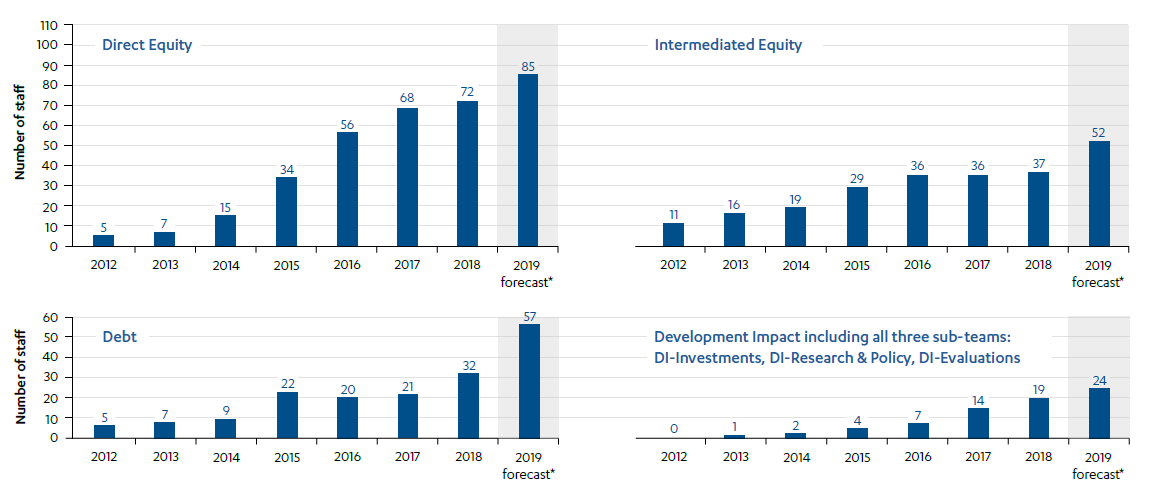
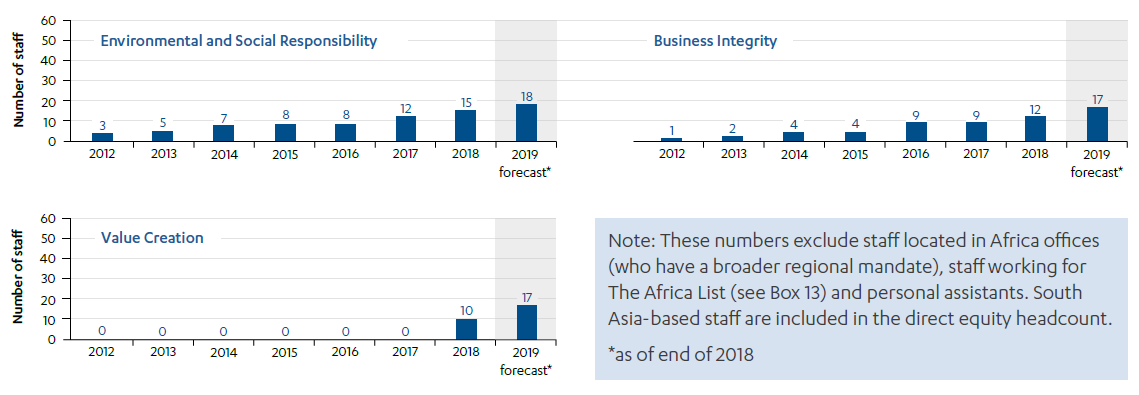
Figure 5: CDC organisational structure
* MedAccess and Gridworks are fully-owned subsidiaries of CDC, attached to the Debt and Infrastructure teams but with their own management and staff
Source: CDC
Before 2011, CDC had operated largely independently of DFID, recycling its financial returns into new investments. During the review period CDC and DFID have begun to work more closely together.
CDC contributes to poverty reduction first and foremost by creating jobs and catalysing sustainable economic growth. It also aims to reduce poverty by improving access to essential goods and services, both directly through investment in private sector service provision and indirectly through its contribution to increasing tax revenues.
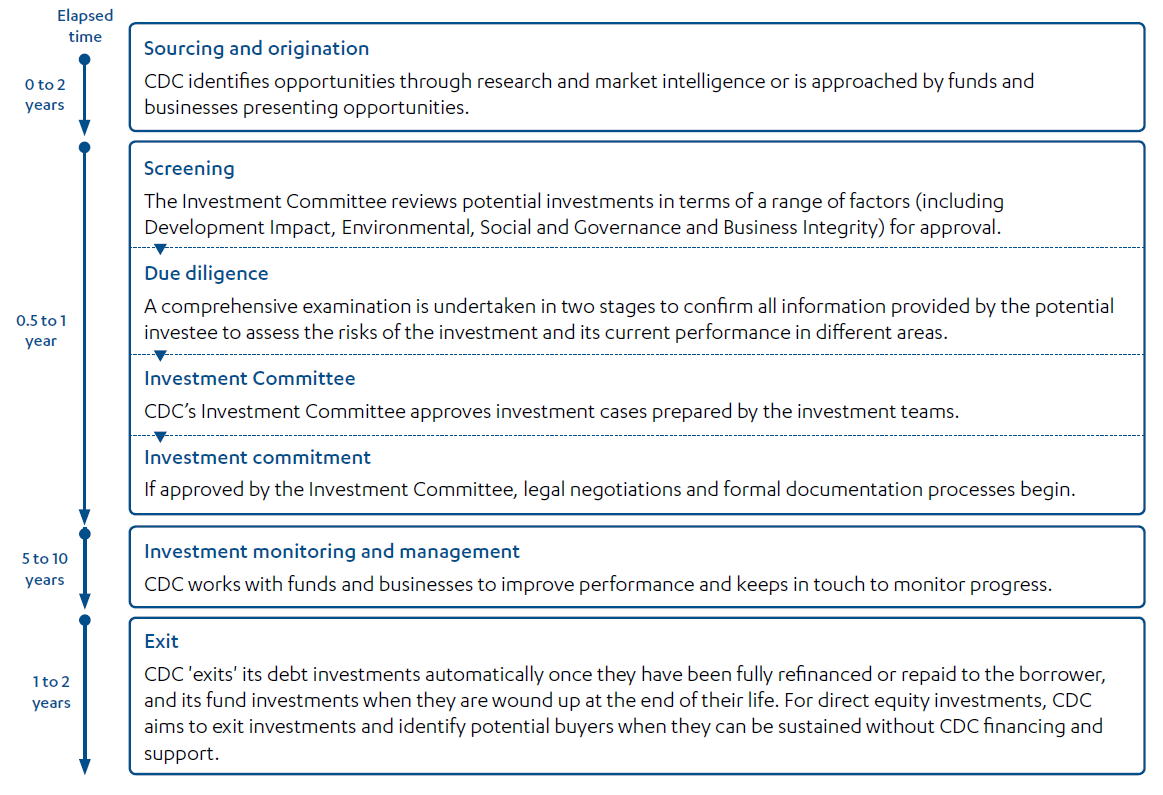
To support its focus on more challenging markets, and priority sectors, in Africa and South Asia (see Figure 2), CDC worked with DFID to develop new criteria for screening and prioritising potential investment, including a Development Impact Grid. This grid is CDC’s primary tool for screening investment opportunities to ensure that it focuses on the countries that are most in need of investment, and on the sectors in those countries that have the greatest potential for job creation (see Box 6 in the Findings section for a more detailed description). Further details of CDC’s investment process are provided in Annex 2.
Recognising CDC’s potential to support its economic development strategy, DFID made a series of investments of new capital between 2015 and 2018 – the first CDC had received for 20 years – totalling £1.8 billion. DFID has committed to further injections through to 2021, by which time CDC’s net assets are projected to grow to more than £8 billion, compared with £2.8 billion in 2012. While DFID has committed £620 million per year of new capital to CDC, with an option to increase this to £703 million per year, the actual amounts drawn down to date by CDC have been lower: £375 million in 2017 and £360 million in 2018.
The objective of these additional commitments was to enable CDC to scale up its investment, while giving it the capacity to accept higher levels of investment risk and lower returns as it moved into riskier markets and sectors. To facilitate this, DFID introduced a separate ‘Catalyst Portfolio’ (alongside the main commercial portfolio, now called the ‘Growth Portfolio’) and also reduced CDC’s overall financial return hurdle to ‘greater than break even’ to encourage CDC to take greater financial risks in return for greater development impact. CDC’s financial return hurdle for the Growth Portfolio remained at 3.5%.
CDC’s new strategic framework for 2017-21 reinforces the organisation’s commitment to maximising development impact in the most challenging markets. The framework includes plans for a series of ‘market building strategies’ to help tackle market failures in specific sectors (as part of the Catalyst Portfolio), as well as new commitments on women’s economic empowerment, job quality and climate change, consistent with DFID’s priorities across its economic development work.
As a result of these developments, the significance of CDC’s role within DFID’s economic development strategy, and in the UK’s aid portfolio as a whole, has grown substantially over the period of this review.
Findings
Does CDC have a credible approach to achieving development impact and financial returns in low-income and fragile states?
In this section we examine the progress that CDC has made between 2012 and 2018 in establishing a coherent strategy for achieving development impact at scale in low-income and fragile states, while at the same time managing a growing portfolio of investments.
There is a clear development case for CDC’s strategic shift towards low-income and fragile states
DFID’s policies for economic development since 2012 and its business cases for the recapitalisation of CDC set out a broad but credible rationale for providing development capital in poorer countries. This is based upon the financing gap in meeting the Sustainable Development Goals, the continuing barriers to private investment in much of sub-Saharan Africa and South Asia (including the high levels of risk faced by private sector investors), and the importance of job creation as a mechanism for lifting people out of poverty.
In our review of DFID’s approach to promoting inclusive growth in Africa, we praised the department’s ambitions for achieving transformative growth and creating jobs at scale, while noting the many practical difficulties associated with this. Development capital plays a central role in these ambitions.
Within the literature and in the countries we visited, we found strong evidence of the need for additional capital – in particular for ‘patient’ capital that is invested for the long term, without the expectation of early returns. CDC investees and external experts identified the high interest rates on bank lending and the limited availability of longer-term loans in countries such as Nigeria and Malawi, as well as the relatively underdeveloped private equity markets across Africa, as barriers to the growth of small- and medium-sized enterprises (SMEs). There is consequently strong demand for support from development finance institutions (DFIs) such as CDC, which offer finance on terms that are generally more favourable than those offered by commercial banks and investors, often in combination with the provision of technical assistance.
In sub-Saharan Africa, countries such as Nigeria and Kenya have seen growth in their private equity markets in recent years (Kenya shifted from B to C in terms of CDC’s categorisation of investment difficulty over the review period). However, there are sharp regional variations within countries. In Nigeria, for example, experts told us that private equity investment was concentrated in Lagos and Abuja, as well as in sectors such as property and infrastructure. Growth in investment markets remains constrained by risk factors such as currency volatility, falling commodity prices and unhelpful financial regulation. We heard from a country representative of the International Finance Corporation (IFC) that private equity funds in sub-Saharan Africa consequently face challenges in raising finance from private investors.
CDC’s shift in strategy also helps to respond to successive concerns raised by the National Audit Office (NAO) and the International Development Committee (IDC) that CDC’s investment in middle-income countries may not have been fully benefiting the poor, and risked displacing commercial investment (see Box 5).
There is therefore a strong case for the decision to refocus the CDC portfolio towards low-income and fragile states. Nonetheless, it is also clear that investing at scale in these much more difficult markets and delivering development impact and financial returns where these are often difficult to predict has involved significant new challenges for CDC.
Since 2012, CDC has successfully reoriented its investment activities more towards low-income and fragile countries
CDC’s plans for the period of this review reflect a progressive focus on low-income and fragile states. CDC’s strategy for 2012-16 was to invest exclusively in Africa and South Asia, with an aspiration to shift CDC’s capital to more challenging regions over time. The more recent strategic framework, covering the period 2017-21, commits CDC to increasing the volume of its investments in poorer and more fragile countries and regions, where its “capital is most needed”. DFID’s 2015 and 2017 business cases for new investment in CDC also reaffirm CDC’s commitment to investing in fragile and conflict-affected countries.
The introduction of the Development Impact Grid in 2013 has played an important role in helping CDC to focus new investment on low-income and fragile countries. By weighting countries according to their level of investment difficulty, the grid provided a means of encouraging investment towards poorer countries. The grid includes 33 fragile and conflict-affected countries (according to DFID’s classification), which in most cases are both low-income and high-risk (the exceptions being Egypt, Bangladesh, Kenya and Cambodia). The grid also provides a simple but useful tool for encouraging investment in sectors with the greatest potential for job creation in these countries (see Box 6).
Box 6: CDC’s Development Impact Grid
In order to strengthen the development impact potential of its investment activities, CDC worked with DFID to develop a Development Impact Grid, an investment screening tool that scores potential investments based upon country and sector characteristics. The grid was designed to guide investment to those countries and states most in need of finance and those sectors most likely to create jobs and economic growth.
Country ranking: The grid divides the countries and Indian states in which CDC invests into four categories of investment difficulty – from A to D, with A being the most difficult investment environment (see Figure 2). It measures investment difficulty by applying an equally weighted index combining five indicators: (i) market size, (ii) income level, (iii) available credit to the private sector, (iv) ‘doing business’ rankings of the regulatory environment for the private sector and (v) a composite measure of state fragility designed by DFID.
Sector ranking: The grid divides CDC’s priority business sectors
into three categories of job creation potential – high, medium
and low, depending on their propensity to generate employment
directly or indirectly (see Figure 2).
It then combines the sector and country rankings into a score from 1.00–4.00, based upon the matrix shown here. DFID set CDC an overall Development Impact hurdle score of 2.4 in 2012 and 2017.
CDC is now more geographically concentrated on difficult markets, including fragile and conflictaffected states, than other DFIs. In our interviews with external stakeholders, including other DFIs, economic think tanks and civil society organisations, CDC’s reorientation towards more challenging markets and greater development impact was both recognised and welcomed.
New investment products, increasing staff capacity and lower financial targets have facilitated CDC’s reorientation towards low-income and fragile states
In order to successfully expand its portfolio into more challenging and complex markets, CDC recognised that it must work harder to find suitable investments, provide its investees with a broader range of support and manage its portfolio in new ways. CDC’s 2012-16 strategy set out plans for introducing new investment products and building up its staffing levels and expertise. DFID supported this reorientation towards riskier markets by lowering CDC’s financial targets.
A key part of CDC’s transition strategy was to diversify its investment products to include direct equity and direct debt funding, in addition to indirect investments through private equity funds. Between 2012 and Q3 2017, 61% of all new CDC investments were made through direct equity and 22% through direct debt, with only 17% through funds. There was strong agreement among those consulted for the review that this shift has given CDC more flexibility to respond to the needs of businesses, including early-stage SMEs, in more difficult markets in Africa. Reflecting this, we found that CDC’s direct investments have higher average Development Impact Grid scores than its indirect investments via funds.
Figure 6: Composition of the portfolio by investment type
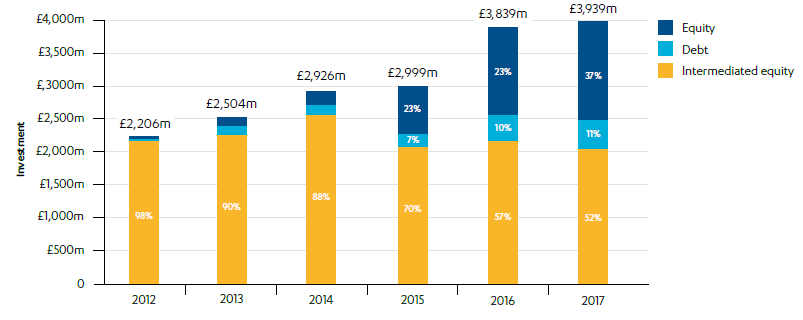
Source: Annual Accounts 2017, CDC Group plc, p. 5.
To enable it to deliver these strategies, and in particular to originate and manage direct investments, CDC has significantly expanded its management and operational capability. Staff numbers have increased from 47 employees in 2012 to 308 by July 2018, with 79 staff now working on direct equity. CDC nonetheless told us that it had underestimated the time that it would take to build up the resources required to implement its new strategy. Progress had therefore been slower than planned, for example on building the direct debt team. CDC plans to continue building its resources and capability, aiming to employ 450 staff by 2021.
To facilitate greater risk-taking in pursuit of development impact, DFID has progressively reduced CDC’s financial return targets. Before the review period, CDC’s target for financial return was 5%. From 2012, CDC was required to achieve a minimum ten-year average return of just 3.5%. This enabled CDC to build up a higher-risk portfolio and pursue investments in more challenging markets and nascent sectors, with lower short-term returns but long-term growth potential. The 2017 Investment Policy left the existing ‘profitability hurdle’ for the Growth Portfolio in place (a ten-year average return of at least 3.5%) but also introduced a second, lower profitability hurdle for CDC as a whole, requiring the Growth and Catalyst Portfolios taken together to achieve a positive net profit (in other words a return of more than 0%), measured over a ten-year period. Depending on the relative size of the two portfolios, these two hurdles would therefore allow the Catalyst Portfolio to operate at a significant loss.
CDC is piloting some innovative financial instruments, but is yet to develop a clear and comprehensive strategy for identifying and supporting opportunities in challenging markets
In building up its portfolio in low-income and fragile states, a key challenge facing CDC is in finding a sufficient pipeline of suitable businesses in which to invest. The economies are typically smaller, the business environment is more challenging and many firms do not meet CDC’s stringent environmental, social and governance (ESG) standards. CDC is therefore required to take a more active approach to identifying and developing new investment opportunities.
In the poorest and most fragile states investable opportunities are rare, and often have to be created, sometimes over many years… as countries become more developed, investable opportunities increase.
Investing to transform lives: Strategic framework 2017-2021, CDC, 2017.
CDC is piloting some innovative financial instruments that it hopes will increase its ability to operate in more challenging markets:
- Platform investments, through which a single investment by CDC can support multiple businesses. Under this model, CDC makes a direct equity investment in a company which it knows and trusts in one of its priority sectors. This new capital enables the investee to invest in other opportunities in the sector, often in different countries (see Box 10 on CDC’s investment in Globeleq).
- Permanent capital vehicles, which are a means of making longer-term equity investments beyond the standard ten-year private equity model, in order to help businesses grow in difficult markets. CDC’s first investment in a permanent capital vehicle was made in 2017, with a $20 million investment in Solon Capital Holdings in Sierra Leone. Solon Capital Holdings has since made investments in two of CDC’s priority sectors – education and construction – among others.
- Risk-sharing facilities, designed to increase small business access to commercial finance. The first such facility was an innovative $50 million partnership with Standard Chartered Bank in Sierra Leone (see Box 7).
- A supply-chain finance initiative, which aims to improve the cash flow of SMEs within domestic supply chains in Africa and South Asia, again in partnership with Standard Chartered Bank. In August 2018, the first supply chain facility was approved ($150 million, of which CDC contributed $75 million). Suppliers in Nigeria and Ghana will be the first to benefit from the programme. Other countries are also in the pipeline.
- A new £65 million grant facility available to all investees in the Catalyst and Growth Portfolios to access technical assistance support, as well as for testing solutions to systemic issues affecting multiple CDC investees, for example in relation to environmental sustainability or gender issues.
Box 7: Innovative support for SMEs through a risk-sharing facility in Sierra Leone
In response to the Ebola crisis in Sierra Leone in late 2014, CDC and Standard Chartered Bank developed a risk-sharing facility to provide SMEs access to capital that was unavailable in the country at the time. Through the risk-sharing facility, CDC assumes a share of the risk of financial loss alongside Standard Chartered Bank. This allowed the bank to lend the larger amounts necessary to keep SMEs operating through the crisis.
The original facility provided $26 million in working capital to nine companies, enabling them to scale up the supply of essential consumer items (including staples such as rice, flour and cooking oil, hygiene products and building materials) in areas where supplies had been badly affected by the Ebola crisis. The facility was renewed and expanded in 2016, 2017 and again in 2018 following these early successes, with $33 million provided in 2018 to 13 companies. The expected benefits include job creation and higher levels of trade.
Although individually promising, we are concerned that these innovations are unlikely to drive the scale of investment and development impact that CDC is seeking in low-income and fragile countries without being underpinned by a more comprehensive strategy or approach for sourcing investment opportunities and supporting investees in the most difficult markets.
CDC is moving towards a stronger sector focus, but could be more transformational in its approach
DFIs such as CDC aim to achieve their most important development impact by unlocking private sector investment, building markets and promoting the transition towards more productive economies. Successive DFID economic development strategies and business cases for CDC, as well as CDC’s own strategies and plans, have emphasised this catalytic role. In its 2017-21 strategic framework, CDC asserts that “life-changing progress comes from growth that transforms economies” and commits to investing “to transform whole sectors”.
From 2013, the Development Impact Grid encouraged CDC to focus its investment on specific sectors that create the most jobs. CDC’s 2017-21 strategic framework confirmed that CDC will focus on seven priority sectors: construction, education, financial institutions, food and agriculture, health, infrastructure and manufacturing. To support this sector focus, CDC has produced a variety of market analyses, investment criteria and some strategy documents for a limited number of sub-sectors. However, it has been slower to develop comprehensive sector strategies to guide its investment teams and help support more transformational impact, working with other partners.
In 2017, CDC introduced a range of ‘market building strategies’ under its Catalyst Portfolio in an attempt to support more transformational change. The initial pilot strategies covered a limited number of specific sector priorities, including access to medicines and other health commodities, energy and climate change adaptation. DFID told us that they have asked CDC to be even more ambitious with its investments under its Catalyst Portfolio.
One example where ICAI believes CDC could show more ambition is in its Off Grid Solar strategy. This is helping to improve access for the approximately 1.2 billion households that lack electricity worldwide, but is focused on the pay-as-you-go home solar sector, where there is existing demand from lower-middle-income consumers and interest from other investors. Reflecting this, CDC also invests in this sector under the Growth Portfolio. CDC’s investments under the Catalyst Portfolio are distinguished by providing riskier local currency debt loans, to help support the sustainable growth of the nascent sector. CDC says that it is also investing in financially riskier and larger-scale mini-grids, which the World Bank currently invests in to help bring power to poor rural communities, through other strategies.
CDC now has plans to develop comprehensive strategies for its seven priority sectors in 2019, which will set out how it will build, manage and monitor a portfolio of impactful investments (including through market building activities) in each sector. Sector specialists are being recruited into CDC’s direct equity team and it is expected that they will work closely with DFID’s sector specialists.
We welcome these important developments but believe that more could have been done earlier in key sectors to help drive transformational change. A number of commercial fund managers and academic experts we consulted also thought that CDC could have done more to address specific development challenges and capital constraints in sectors such as healthcare, agriculture and affordable housing, and to encourage transformation, working with country governments and other DFIs.
CDC has been slow to build its country presence outside of India, and to develop geographic strategies or priorities
CDC has been slow to build a country presence in its priority markets. From 2013, CDC re-established offices in India, and has since developed closer interactions with DFID as a result. In 2013, CDC also hired its first Regional Director for Africa, charged with supporting its expansion into direct equity and debt investments across the continent. The 2016 NAO report emphasised the importance of CDC expanding its physical presence in Africa and South Asia, but noted that CDC did not yet have a fully developed plan for expansion. At the end of 2017, out of 266 CDC staff, ten staff were based in India, but only seven in the whole of Africa.
The wide cross-section of expert stakeholders that we spoke to consider a strong in-country presence important for engaging with SMEs, originating investment opportunities and supporting active portfolio management to help firms succeed and create development impact.
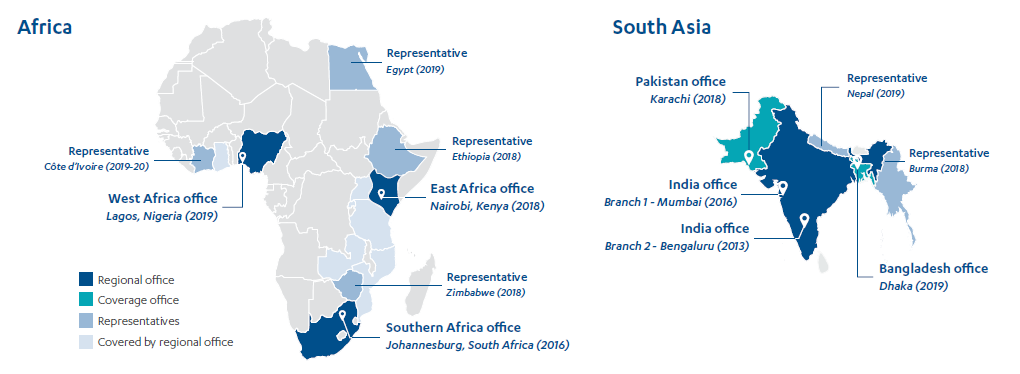
CDC now has firmer plans in place to expand its overseas presence. It has prepared an Africa Coverage Strategy, which sets out how its Africa personnel will support CDC’s investment agenda in these more difficult markets, and is projecting 33 employees there by 2021, alongside 43 in South Asia. The aim is to replicate the capability of CDC’s offices in India across its office network.
Plans for Africa currently involve regional offices in Johannesburg (established in 2016), Lagos and Nairobi, and single representatives in Zimbabwe, Ethiopia, Egypt and Côte d’Ivoire. The selection of countries took account of portfolio management needs, market potential, development needs, the UK government’s existing footprint and accessibility. However, initial plans for a representative based in the Democratic Republic of Congo were dropped when the nominated employee moved to Ethiopia. CDC says that it intends to expand to four or five more countries in the next five years.
Figure 7: CDC planned overseas presence and coverage 2018-2021
We recognise the significant challenge of building an effective local presence in difficult markets, particularly at a time of considerable change and expansion throughout the organisation in the UK. But we believe that more could have been done earlier, given the emphasis on growing direct investment in low-income and fragile states, and the subsequent capital increase approved by DFID. CDC made direct investments in Africa totalling $1.6 billion between 2012 and 2017. CDC’s weak country presence there has meant that these investments have been largely unsupported by country-based staff.
We consider the expansion of a strong country presence to be an urgent priority for CDC. Failure to do so could undermine plans for the continued scale-up of CDC’s investment activities in Africa and the broadening of its development impact there.
CDC’s 2017 strategic framework notes that the significant differences in investment readiness between countries requires a tailored approach. An internal strategy document from 2016, concerning CDC’s investments in fragile and conflict-affected states, outlined plans to foster transformational growth at country level by coordinating multiple investments in key sectors, as CDC did in Sierra Leone following the Ebola crisis when it developed a risk-sharing facility with Standard Chartered Bank (see Box 7). However, CDC has not prepared detailed strategies or plans for any individual country or geography. Instead, CDC is now producing ‘country perspectives’ for key markets, based upon a synthesis of economic data and consultation with DFID.
We recognise the difficulty of producing comprehensive plans without a strong local presence. However, we see considerable value in developing a more comprehensive analysis of the investment challenges and opportunities in individual countries or geographies, ideally in conjunction with the country governments and with DFID and other DFIs and development partners, and agreeing shared priorities to help improve the investment climate, build markets and guide investment.
CDC has moved from a narrow focus on job creation towards a broader understanding of development impact, but there is more work to do to fully operationalise this
CDC’s primary method of selecting investments with the potential to deliver development impact in low-income and fragile countries is to prioritise sectors with the greatest potential for job creation. From 2012, DFID encouraged CDC to introduce a strong focus on jobs as the primary route to poverty alleviation, given for example that the rate of job creation in Africa is well below the growth rate of its labour force. Working with DFID, CDC commissioned an analysis to identify sectors with a higher propensity to create jobs, and then designed its Development Impact Grid to prioritise these. It has recently updated this analysis with fresh data (see Figure 8).
Figure 8: CDC’s priority sectors

By focusing narrowly on job creation, CDC may have missed opportunities to maximise its development impact. A report commissioned by DFID in 2016 expressed a concern that “one possible disadvantage [of the grid] would be if it led to an excessive focus on jobs at the expense of other areas of development impact”. While it concluded that CDC used the grid flexibly in selecting its investments, the report recommended that additional development impact areas should be tracked. Some external stakeholders we interviewed also suggested that CDC should give more consideration to addressing economic inequality (including across geographical areas and between social groups), to help ensure that CDC’s investments benefit the poorest.
CDC now recognises the need for a broader approach to development impact. Its 2017 strategic framework considers development impact at three levels – people and communities, companies and local economies, and broader capital markets (covering mobilisation). There is a stronger emphasis on the wider contribution of CDC’s investments to poverty reduction and gender equality, including through providing a clearer articulation of the links with the Sustainable Development Goals (see Figure 9). CDC’s development impacts are to be achieved primarily through a combination of job creation, sector effects and the introduction of four ‘strategic initiatives’ – women’s economic empowerment, climate change, job quality and skills and leadership.
Figure 9: How CDC aims to contribute to the SDGs
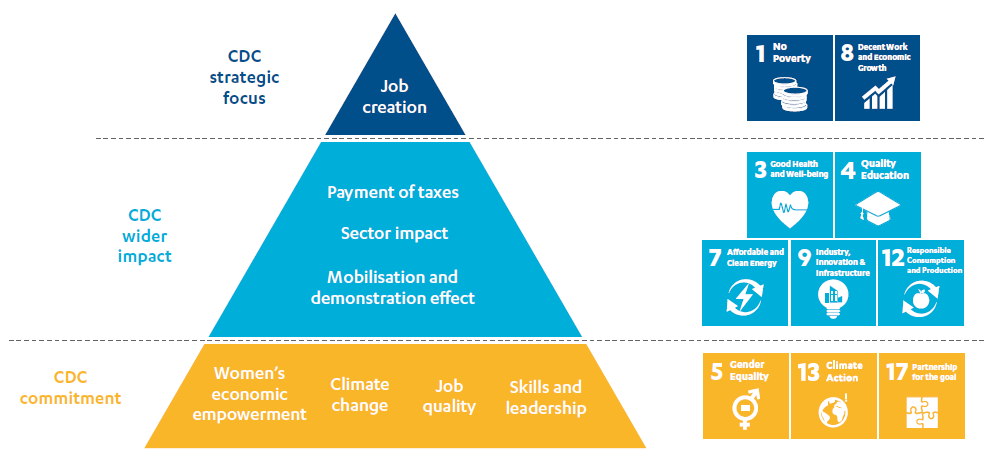
Source: CDC strategic framework 2017-21.
To support this broader emphasis, CDC has embedded 12 development impact professionals in its investment teams, with recruitment under way for two further posts. Since January 2018 these staff have been responsible for formulating a more comprehensive ‘development impact case’ for each potential investment at the screening stage, and for identifying appropriate performance measures to help monitor and manage the impact of CDC’s investments throughout their lifecycle. CDC’s Development Impact team (alongside the E&S and Value Creation Strategies teams) now report to CDC’s newly appointed Chief Impact Officer, who sits on CDC’s executive committee. These improvements should enable CDC to better understand and enhance its development impact.
There is more work to do to fully operationalise this new thinking on impact across CDC’s investment practices. The development impact case is a largely qualitative narrative, and CDC’s accompanying Investment Process Overview (2018) does not set out how evidence of development impact should be weighed against other investment criteria. CDC does not yet have a consistent set of wider development impact measures, beyond the grid score and a limited set of sector metrics, that could be systematically applied to its investments and help guide the decision-making of investment managers from deal origination through to approval.
A number of other DFIs score their investments against a wider range of impact factors, including additionality, promotion of corporate social responsibility, and the potential for mobilising other investment finance. FMO, the Dutch DFI, told us that they now specifically ‘label’ whether their investments contribute to Sustainable Development Goal 10 (reducing inequality), and also adopt targets for investment that promote gender equality and smallholders. The IFC recently announced a new assessment framework, the Anticipated Impact Measurement and Monitoring system (AIMM), which takes a comprehensive view of development impact and quantifies potential impact across a range of measures.
Within the scope of this review, it is not possible for ICAI to assess the relative merits of alternative approaches to investment assessment. CDC’s initial rollout of the development impact cases provides an important opportunity for internal and external learning and for refining CDC’s procedures in this area.
As part of its new approach to development impact, CDC is paying closer strategic attention to job quality and gender equality, but there is room for improvement
CDC has addressed job quality over the review period through the E&S team’s compliance requirements, which are based on IFC performance standards and cover issues such as core labour conditions, working hours, pay and grievance mechanisms. Deficiencies are then addressed via a legally binding E&S action plan. The E&S team has also produced several helpful due diligence guides and products over the period.
Although this compliance activity is important, we believe that CDC could do more to strengthen its approach to measuring and supporting job quality, in support of the International Labour Organization’s broader definition of ‘decent work’ and Sustainable Development Goal 8.53 We note that the NAO report of 2016 found that CDC had been considering how to measure job quality since 2012, but without making much progress. By 2018, CDC told ICAI that its strategic initiative on job quality was behind its newer work on gender, and that it had not yet completed its strategy for this area. CDC continues to engage with other DFIs on this issue, as part of the Let’s Work Partnership administered by the World Bank.
Before 2018, CDC’s objectives related to gender were focused on working with investees to help them comply with the social requirements in its ‘Code of Responsible Investing’, some of which disproportionately affect women. However, we found limited evidence in our sample of investments from this period of objectives specifically related to gender. The 2017 strategy included a new emphasis on furthering women’s economic empowerment, in support of Sustainable Development Goal 5 (gender equality), in keeping with DFID’s economic development strategy. A gender strategy was introduced in 2018 to help raise awareness across CDC of the potential of its investments to promote women’s leadership, job quality and access to finance and services. This also committed CDC to helping to tackle more systemic barriers to women’s empowerment. CDC is continuing to improve its approach to this issue. It recently introduced an investment objective in relation to gender, joining other G7 DFIs in committing to mobilise $3 billion for businesses supporting women.
Building on the non-optional requirements in its E&S Code, CDC currently frames its work on women’s economic empowerment (as well as support for other strategic initiatives such as job quality) as part of its value additionality support. Different aspects of value additionality are pursued where specific opportunities are identified, rather than being scored or assessed systematically as part of producing each development impact case. This targeted approach is a helpful initiative to focus efforts but may miss opportunities that a more comprehensive approach might identify. CDC says that it recognises some of the tensions and overlap between its development impact and value additionality work and is looking to further harmonise its approach.
CDC has developed some investment instruments to target the poor, but could adopt a sharper focus on poverty reduction across its portfolio
In an effort to target the poorest in society, DFID appointed CDC to manage two new investment vehicles, the Impact Fund and the Impact Accelerator, in 2013 and 2015 respectively. In September 2017, these DFID funds were transferred onto CDC’s balance sheet, as part of the Catalyst Portfolio. Both are designed to invest in businesses that provide goods, services and income-earning opportunities for vulnerable and underserved groups, or to work in more challenging places (such as conflict-affected areas) with limited investment activity. Investments by these funds are expected to be higher-risk but with long-term commercial potential, and to help catalyse other investments. Investees have access to technical assistance, as well as financial support. There are examples of investments in nutrition, agribusiness, renewable energy and construction in countries such as the Democratic Republic of Congo, Rwanda, Ethiopia, Malawi and Rwanda.
Box 8: Examples of CDC’s Impact Fund and Impact Accelerator
The Impact Fund
- CDC committed $15 million to Novastar Ventures East Africa Fund in 2014. Novastar Ventures is a Nairobi-based venture capital firm, which invests in innovative, early-stage businesses in the education, healthcare, agribusiness, food and water sectors, targeting low-income communities. The fund’s investments include Sanergy, a Kenyan franchise which provides high-quality sanitation facilities in Nairobi’s urban slums, and Bridge International Academies, which operates a chain of low-cost nursery and primary schools in Kenya, Uganda, Nigeria and India.
- In 2017, CDC committed $15 million to the Fund for Agricultural Finance in Nigeria (FAFIN), managed by Sahel Capital, which targets SMEs across the agricultural value chain in Nigeria. FAFIN made five investments in the agribusiness sector in Nigeria between 2015 and 2018, including in a dairy producer and processor, a poultry farm, a cassava starch processing company and a rice producer and processor, which work with smallholder farmers and/or employ local labour. According to Sahel Capital, FAFIN-backed businesses support over 400 jobs directly and more than 1,200 indirectly. Of the direct jobs supported, 77% are taken by women and young people. One of these investments is located in northern Nigeria, where there is limited investment activity.
The Impact Accelerator
- Agricane is an agricultural engineering and development company founded in 1996. It owns three farms totalling 3,700 hectares of land in Malawi. CDC invested $5.5 million in 2017 to help the company set up remedial irrigation works in a commercial sugar cane plantation, to address soil salinity problems. The investment helped preserve 88 permanent and 150 seasonal jobs. There is the potential to develop a platform relationship with Agricane, which would allow CDC to establish a pipeline of investments in Malawi without requiring its own local presence.
Though innovative, these two investment vehicles remain small in scale compared with CDC’s Growth Portfolio. In 2017 they accounted for just 6% of CDC’s new commitments.
Figure 10: Composition of CDC’s overall portfolio, 2018 (%)
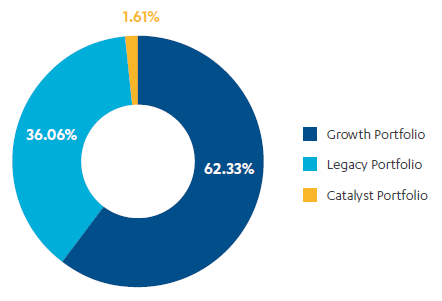
Beyond the Impact Fund and Impact Accelerator, we found mixed levels of engagement in CDC in relation to the challenge of reaching the poorest. The latest direct equity strategy includes an objective to support businesses that serve the poor and that work in poorer regions, alongside companies with the potential for growth. There is no explicit reference to the poor in the objectives of CDC’s other product strategies, although the intermediated equity strategy does make reference to supporting companies graduating from the informal economy. Some of the CDC staff we interviewed thought that CDC could use its influence as an investor more to encourage pro-poor initiatives in investee companies, for example where CDC has board representation as a result of a direct equity investment or where it is co-investing alongside a fund investment.
In our investment sample we identified a number of possible opportunities to increase the pro-poor focus of individual investments which had not been actively encouraged by CDC. For instance, in Nigeria we found promising initiatives around corporate social responsibility that had not been fully implemented or sustained, and innovative ideas for providing products and services to underserved areas that had not been pursued. We also saw scope for more proactive support for women’s employment, particularly within sectors and occupations where women are under-represented. Some of these examples related to intermediated equity investments through fund managers. In these cases, CDC does not ordinarily have a direct relationship with investees, making it more difficult to influence their strategy and practices.
Positively, CDC’s new development impact professionals have been tasked with helping investment managers with ‘impact management’. This includes identifying opportunities to enhance impact throughout the investment lifecycle, as well as improving CDC’s monitoring of development impact.
Until very recently CDC has had no overarching strategy for encouraging the mobilisation of private finance
DFIs achieve development impact at scale by demonstrating that commercial investments are viable in sectors and areas neglected by the market, thereby unlocking larger financial flows. This is particularly challenging in low-income and fragile states, where there are fewer sources of private capital to influence.
CDC has no overarching strategy for mobilising private finance. Its 2017-21 strategic framework includes mobilising private capital among its seven key goals, but it only talks in general terms about how CDC will look for new ways to do this, and there are no specific plans for difficult markets. DFID suggested that CDC put in place a specific strategy for mobilising private finance by the end of 2018. CDC recently confirmed that it had submitted a proposed strategy to its Board in November 2018.
There is more detail in the individual product strategies, but the emphasis on mobilisation varies, and there are some important gaps and inconsistencies. CDC’s direct equity strategy discusses multiple ways of mobilising capital. These include improving ESG standards to make businesses more ‘investment-ready’, actively seeking out co-investors, and attracting larger financial institutions such as pension funds. The strategy projects that CDC may ‘exit’ four to six direct equity investments by 2021, providing an opportunity to involve new private sector investors. The timely identification of candidates for exit, for example when they have become strongly profitable or cash-generative, requires a regular review of the investment portfolio. CDC told us that they discuss potential exits at its quarterly portfolio review meetings.
The intermediated equity strategy emphasises CDC’s support for the development of sustainable fund management sectors in Africa and Asia. Many stakeholders emphasised the help that CDC has provided to first-time fund managers and its encouragement of nascent private equity markets in several countries in Africa. A report prepared by the Harvard Business School in 2015 provided strong evidence of CDC support for this sector in a number of countries between 2004 and 2012.
CDC’s approach to mobilising capital through direct debt was much less well developed, with limited thinking on how to ‘exit’ loans through refinancing. However, CDC’s new Construction Finance Facility goes some way to addressing this issue in the independent power sector, through the provision of bridging finance (see Box 9).
Box 9: Mobilisation through the Construction Finance Facility
According to the World Bank, two out of three households in sub-Saharan Africa have no electricity connection, in part because of a lack of investment in power generation capacity. One solution to this funding gap is private investment in Independent Power Producers (IPPs), whereby electricity authorities purchase power from commercial investors.
CDC’s new Construction Finance Facility is designed to mobilise private investment in IPPs by providing bridging loans to developers during the construction phase of small to medium-sized power projects. According to CDC’s Debt Investment Strategy (2017-21), delays in IPP projects are often due to complex and time-consuming multi-lender due diligence processes. These delays are often compounded by lengthy negotiations because of the number of lenders involved. By providing the Construction Finance Facility as a sole lender – working with experienced developers with whom CDC has an established track record – delays can be avoided and the due diligence processes streamlined. CDC would then aim to sell down debt after the construction is completed, when there should be stronger interest from commercial lenders. The Facility plans four to six investments between 2018 and 2021, with financial commitments growing to around $80 million per year by 2021.
We found that CDC could work more closely with DFID, country governments and other DFIs to help improve the investment climate. DFID also suggested that CDC could be more transparent and proactive in publishing its performance data, to help build market confidence. CDC told ICAI that they have begun to examine what additional track record information could be published.
CDC and DFID are working more closely together, but there is room for more regular engagement at the country level
While CDC is set up to be operationally independent of DFID, the department continues to agree CDC’s overall investment policy and to influence its priorities through a range of channels. DFID also manages economic development programmes in many of the same countries, creating scope for complementary working.
The relationship between DFID and CDC has improved over the review period. Before 2012, there was no structured interaction other than formal shareholder meetings. In 2012, DFID and CDC started to meet more regularly at senior management level. A Memorandum of Understanding was developed in 2013 to enhance working relationships. DFID intensified its engagement during the development of CDC’s 2017 strategic framework, and CDC’s strategy team and DFID’s private sector development team now meet weekly. DFID is exerting more influence in a number of areas, including CDC’s planned sector strategies, its approach to value additionality, and plans for improved monitoring, evaluation and learning. A CDC-DFID collaboration portal has also been developed to share information online, and joint collaboration guidance has been issued for UK government staff in overseas posts.
Both CDC and DFID staff recognise the potential to strengthen collaboration in priority sectors – for example, CDC’s insights into the challenges faced by its investee companies could help to inform DFID’s work on improving country business climates, and CDC and DFID could work together more on improving regulatory regimes for the power sector. Collaboration to date has largely been through formal, centralised processes, but CDC and DFID plan to encourage joint working in sectors by building working-level relationships between their teams. This should also help with better aligning their sector priorities – on our country visits, we saw examples of inconsistent sector approaches between the two organisations in private sector schooling and real estate.
The 2013 Memorandum of Understanding highlighted the desirability of CDC and DFID country offices working together for mutual advantage. While CDC told us that collaboration in India is working well, elsewhere progress on building relationships has been slow.
But we saw some positive examples of DFID’s economic development programmes supporting the work of CDC in Africa. While these generally reflected ad-hoc engagement, they highlight the potential for greater cooperation between CDC and DFID, to leverage their respective experience and expertise. In Nigeria, DFID provided seed funding for early-stage businesses in the home solar sector, which later received investment from CDC, and separately DFID arranged a briefing from its rural markets programme for a CDC investee on expansion opportunities in high-impact sectors. In Zimbabwe, CDC worked with DFID on due diligence assessments for some recent investments. As CDC scales up its activities and presence in these more challenging markets, it will be important to leverage potential synergies with DFID and other development partners, to help maximise development impact.
DFID and CDC recently developed a framework for cooperation to help maximise their collective impact, which was disseminated around DFID country offices. It includes proposals on sharing data, knowledge and networks, as well as increased consultation around CDC’s emerging sector strategies and country diagnostics. In the countries we visited, DFID staff told us that their relationship with CDC had become more active over the past year, but it was evident that there was considerable scope for further improvement.
While CDC’s profitability target has been lowered, it remains cautious of accepting higher risks to maximise potential development impact
CDC’s current strategic framework notes that DFIs typically achieve lower financial returns than commercial investors at a portfolio level, because they take on higher risk (including regulatory and political risks, and the risks of working with young or inexperienced companies). As CDC moves into more difficult markets, these risks are likely to increase, and higher failure rates and a lower overall return on investment can be expected. As noted above (paragraph 4.14), DFID has reduced its expectations of financial return in order to accommodate this.
In the period immediately before 2012, CDC was focused more on achieving financial returns, and less on development impact, than it is today. However, even after DFID adjusted its financial targets, we found that CDC has generally displayed a preference for safer financial returns over higher-risk investments with more development impact. Many within the organisation told us that it is important for CDC to protect its reputation as a prudent investor, and to minimise the risks of losing public money. Indeed, CDC also said that taking on the Catalyst Portfolio at all was met by some resistance within the organisation, and that taking on greater risk requires significant ongoing culture change.
The latest strategic framework acknowledges that CDC has in recent years turned down potentially high-impact investments because it believed that the financial risks outweighed the potential benefits. CDC reports that to date the largest sectoral exposures within its direct equity portfolio have been to infrastructure (with a particular focus on power) and financial institutions, which it identifies as lower-risk sectors. It notes that this focus on “larger, lower-risk investments (but still with high development impact)” will continue through 2017-21.
It is entirely appropriate for CDC to continue to pay close attention to financial returns. Part of its underlying theory of change is to demonstrate that successful investments are possible in challenging places. However, we found that CDC may need to further recalibrate its risk appetite to achieve its objectives in low-income and fragile states. For the Growth Portfolio, we find CDC’s hurdle score for development impact, 2.4 out of a possible 4 on the grid, to be unambitious. CDC has retained this target for the new strategy period, despite previous performance exceeding it.
CDC also needs to articulate and pursue a more clearly differentiated risk profile for the Catalyst Portfolio, in line with the IDC’s 2011 recommendation to use general investments in developing countries to cross-subsidise more targeted ‘pro-poor’ investments, and to communicate this to the market and potential investees.
Addressing these challenges will require a further shift in CDC’s organisational culture, to ensure that development impact is given the same weight as financial return, consistent with CDC’s twin objectives.
Conclusions on relevance
Since 2012, CDC has made a clear strategic shift away from middle-income countries towards sub- Saharan Africa and the poorest countries and states in South Asia, while prioritising sectors with the greatest potential for job creation. It has diversified its investment products, piloted innovative financial instruments, and introduced a Catalyst Portfolio to support transformational change in more difficult markets. More recently, it has outlined plans to expand its technical assistance offer to investees.
This shift in strategy has necessitated very significant changes in the organisation, resources and culture of CDC. This process of change is ongoing, with much still to do to build the country presence in Africa and to embed development impact thinking in its investment teams and processes. Externally, CDC could be clearer about the differing rationales for the Growth and Catalyst Portfolios, and how it balances financial return with development impact.
CDC is expanding its approach to development impact beyond its previous focus on job creation, taxes and finance mobilisation, as well as a limited set of sector metrics, to include women’s economic empowerment and other development impact pathways. There is further scope to make the appraisal of development impact more systematic.
CDC also needs to press ahead with identifying opportunities for transformative impact, and to develop a more concerted approach to mobilising private finance. It could make more use of its influence as an investor to promote development impact and poverty reduction among its investees. A strengthened collaboration with DFID should help with these challenges, including through supporting wider policy and regulatory reforms.
Overall, we find that CDC has made good progress with refocusing its activities on lower-income and fragile countries, and in transforming the organisation to deliver stronger development impact. However, gaps remain, and many initiatives are at an early stage. This merits an overall green-amber score for relevance, though we urge CDC not to underestimate the magnitude of the changes still required to achieve its objectives.
How effective are CDC’s investments in low-income and fragile states?
In this section, we examine the effectiveness of CDC’s investments made in the period from 2012, when it shifted its strategic focus towards difficult markets in low-income and fragile states. We look at CDC’s effectiveness in achieving both development impact and financial returns. We draw on our assessments of the sample of investments made during this period, as well as on our review of the literature, strategic-level documentation, data and interviews.
CDC has made progress in increasing its investments in low-income and fragile states, but struggles to find direct investments outside a small number of countries
Between 2012 and Q3 2017, CDC made $3.04 billion of new investments through its Growth Portfolio, and $78 million through its Catalyst Portfolio. The Development Impact Grid successfully steered CDC’s Growth Portfolio towards more difficult investment markets in Africa and South Asia. 52% of new investment was made in the most difficult markets (A and B countries and Indian states in the grid) compared with 23% between 2009 and 2011. The proportion invested in the least difficult markets (D countries and states) went down from 43% to 21% between 2012 and 2016.
A recent study also showed that a much higher proportion of CDC’s investments have been in fragile and conflict-affected countries (43%) compared with other leading DFIs. The French DFI, Proparco, is the second-most active in fragile countries, at 28%.
Following significant growth between 2013 and 2015, the proportion of new investments made by CDC in A and B countries and Indian states declined in 2016, and again in 2017, from a peak of 66%. New investments in A countries and states also plateaued in absolute terms, at around $150 million per annum (see Figure 11), despite the large increase in overall investment levels in 2016 following DFID’s first injection.
Figure 11: Distribution of capital disbursements according to country investment difficulty
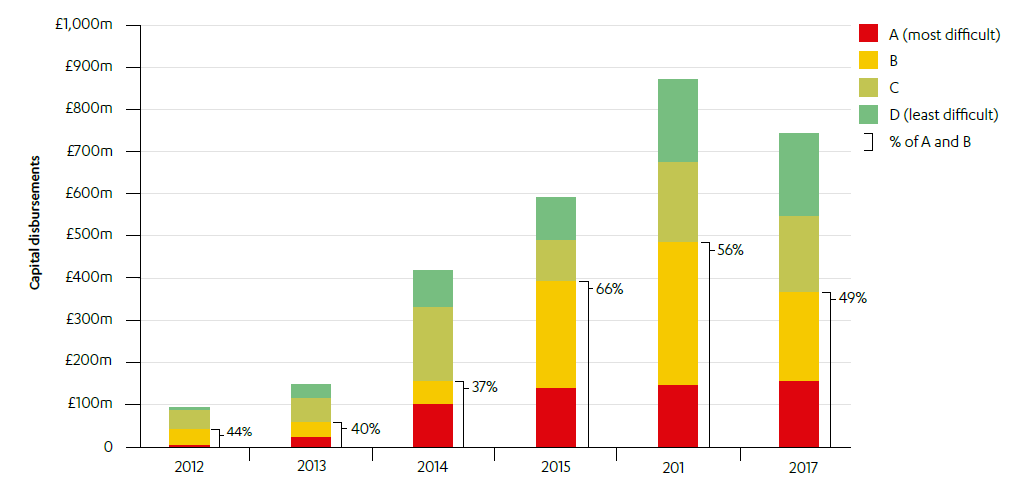
Source: Forward with purpose, CDC Group plc Annual Report 2017.
We also found that CDC’s new investments in A and B countries were heavily concentrated in a small number of countries. CDC can invest in up to 33 countries on DFID’s list of fragile and conflict-affected states. However, 95% of CDC’s portfolio, as of 31 March 2017, was in ten of these countries, while 80% was concentrated in just five of them – Nigeria, Kenya, Pakistan, Côte d’Ivoire and Cameroon – including some of the least poor and fragile of the countries on DFID’s list.62 CDC’s disbursements in A and B countries have also tended to be concentrated in a small number of larger companies and funds. These include Globeleq, CDC’s single-largest direct investment (see Box 10).
India continues to be an important market for CDC – 31% of new investment under the Growth Portfolio ($905 million) was deployed in India between 2012 and Q3 2017, a similar proportion to the 2009-11 period. In a 2017 strategy document, CDC noted a worry that any decrease in disbursements to India might not be made up through investments elsewhere. Over 2012 to 2017, CDC was less successful in investing this capital in A and B states in India (29%), compared with its investment in A and B countries overall (52%).
CDC told us that it has faced two principal challenges in sourcing deals at scale in the poorest countries and Indian states: firstly, a limited supply of funds and viable businesses to invest in responsibly (and particularly in certain sectors), and secondly, a lack of sufficient country presence to help source and support making more direct investments.
CDC has increased its investments in priority sectors overall, although this growth is concentrated in financial services and infrastructure
CDC has made good overall progress in sourcing investments in its seven priority sectors. Between 2012 and Q3 2016, 78% of new investment was made in priority sectors, compared with 54% in 2009-11. By Q3 2017, CDC had made just under $2.6 billion of new investments in its priority sectors. The remaining capital was invested in trade, communications, business services and extractives, largely by generalist fund managers.
Some sectors have received considerably more investment than others. There was much faster growth in financial services and in infrastructure (and particularly the energy sector), which CDC identifies as enablers of private sector development, than in more traditional development sectors such as health, agribusiness and education. The proportion of CDC’s investments held in manufacturing, a sector seen as critical to Sub-Saharan Africa’s future growth prospects, declined over the period (see Figure 12).
Figure 12: CDC portfolio split by priority sector in 2011 and 2017*
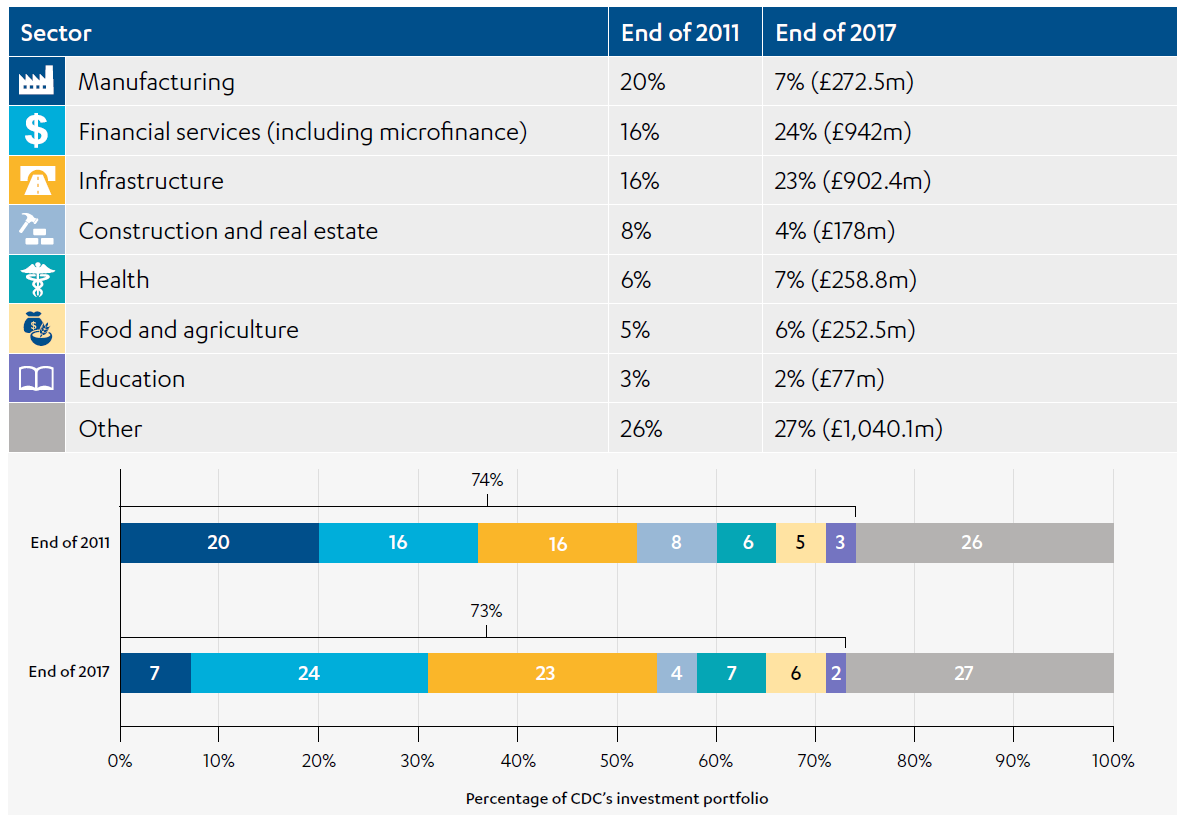
*Data covers CDC’s total portfolio, including all existing and new investments made up until end 2011 and end 2017 respectively.
Source: Steering Group paper on priority sectors, CDC, February 2017, unpublished, and latest CDC investment data.
CDC’s sector split reflects general patterns of investment across DFIs, and confirms findings from the literature that DFIs tend to have fewer investments in sectors with the strongest evidence of poverty reduction or pro-poor growth. Kenny et al concluded that DFIs might better focus on investing in large infrastructure and manufacturing projects, where they have a comparative advantage and can deliver greater development impact (rather than in sectors where it is “comparatively straightforward to put together deals”).
CDC faces particular tensions in investing in financial services, its single biggest sector with over 60 new investments made between 2012 and Q3 2017. CDC has a strategic commitment to increasing access to credit among underserved clients, including through funding banks and other financial institutions in difficult markets. However, it also acknowledges that many DFIs have pursued suboptimal strategies in this sector, with small firms not always benefiting from increased lending. Over the review period, CDC’s two largest financial services investments (constituting just over 40% of all capital disbursed in the sector) were made in institutions in India. CDC’s research into one bank investment in India found that the majority of its lending to SMEs did not result in any direct job creation, although firms benefited from productivity gains. While CDC made proportionally fewer new investments in financial services in 2017 than in 2012, it is concerned that any significant further reduction would have a negative impact on its investment pipeline.
CDC says that it has struggled to find large, viable direct equity investments in Africa, and particularly in sectors such as manufacturing (with 20 investments made over the period). Further illustrating this, CDC’s single largest investment in manufacturing, ARM Cement in Kenya (in which CDC invested $140 million in 2016 to help protect 3,000 jobs), was facing significant difficulties at the time of the review. This transaction accounted for more than 60% of the total of $225 million invested in manufacturing overall. Within health and education (where CDC made 20 and nine investments respectively), CDC told us about some innovative investments in Sierra Leone, Nigeria and Kenya, but also said that large investable businesses in these sectors in Africa are scarce.
Three of the most recent sector-specific sub-strategies in the Catalyst Portfolio got off to a slow start. No investments were made under MedAccess, Transmission and Distribution and the Resource Efficiency Fund in 2017. CDC had forecast investment in these strategies totalling $120 million in 2017. We note, however, that $100 million was disbursed under the MedAccess strategy early in 2018.
CDC does not always do enough to ensure the additionality of its investments
CDC aims to mobilise private sector funding, not crowd it out. Its investments must be ‘additional’ to the market – offering finance and support when it is not available from the private sector, and where possible working as a catalyst for further private sector investment. According to CDC’s own analysis of investments made since 2014, 89% of commitments over the period 2014-17 were financially additional, with the remainder of commitments justified on the grounds of value additionality (in other words the business and other non-financial support that CDC provides to its investees).
CDC reviews financial additionality as part of its investment screening and approval process, although, according to CDC’s additionality guidelines from 2017, formal ‘proof’ is not required. It is generally acknowledged that there is no way to obtain definitive evidence of financial additionality before making an investment decision. However, there is a wide range of evidence that could be gathered in a systematic way to support a more robust assessment.
Our case study visits raised concerns over whether some of CDC’s investments were sufficiently additional. For example, in one case study country, some investees we spoke to said that they would have been able to access mainstream finance in the absence of CDC support, although on less favourable financial terms (and without the support provided by CDC to improve ESG standards). In another of our case study countries, a private equity investor told us that their organisation had been outbid by CDC on one transaction. It is not possible for us to confirm the validity of these claims or assess how widespread this issue might be. However, these examples mirror concerns raised in the 2011 IDC report, in the literature we reviewed and in our discussions with external stakeholders, that DFIs generally do not pay enough attention to the issue of additionality.
CDC is prepared to make an investment which is not financially additional if it believes that it could provide non-monetary support services that are additional to what the commercial market would provide. CDC’s current approach to providing evidence of this ‘value additionality’ would be strengthened by linking this back to the development impact case, and any opportunities and risks related to delivering greater development impact identified at the screening stage.
CDC’s assessment of potential development impact has often been superficial, although this is now improving
It is at the investment selection stage that CDC has the greatest ability to promote development impact, through the choices that it makes. However, in our sample of investments we found that CDC’s consideration of potential development impact consistently lacked depth.
The main documents used by CDC’s Investment Committee to inform investment decision-making said little about potential development impact in comparison with other issues. The information on impact at the level of people and communities for five investments out of 19 (all of which were investments in funds under the Growth Portfolio) was limited to a brief consideration of the grid score, followed by one or two sentences exploring the job creation potential of the pipeline of investees, alongside a focus on financial performance and ESG. The papers for four further investments did not mention impacts for people and communities at all.
Use of evidence to back up development impact assumptions (beyond the grid score) was lacking in the majority of Investment Committee documents. For example, a document for a real estate fund investment in Africa included a projection by the fund manager that it would create a very high number of jobs (22,500) – much higher than the actual number of jobs created by the investee to date. Although CDC tracked the employment created, this projection was not referred to again in other documentation once the investment had been made. Furthermore, the investment ended up benefiting groups towards the top end of the agreed income spectrum.
We also commonly found insufficient attention paid to the socio-economic groups that would benefit from the investment. The Investment Committee papers for more than three-quarters of our sample did not consider this issue. For example, the papers for an investment in an Indian fund that targets healthcare businesses argued that the fund would improve healthcare affordability but did not consider which groups would benefit. CDC subsequently told us that the fund’s initial commitment to target 50% low-income households was an ambition rather than a requirement, and that funded services have largely reached those on above-average incomes. More positive examples in our sample, where issues of equity were considered in more depth, included a fund in Kenya that aimed to support firms targeting slum dwellers, and funds in India and Nigeria supporting firms that source their agricultural products from smallholders in poor states.
CDC began producing development impact cases in 2018, and these are now considered by the Investment Committee. CDC showed us one example of a development impact case included in its final Investment Committee papers for a manufacturing business. This represented a significant improvement on previous investment documentation, with greater consideration of existing data, relevance to the national context and wider development impact. However, weaknesses and gaps in the case suggest important areas for further improvement.
The case referenced promoting inclusive growth as one of two main objectives, and highlighted the critical risks to this (including weaknesses in domestic distribution), but did not propose any risk mitigation strategies for these. CDC told us that it decided to tolerate these risks. There was no mention in the case of how value additionality or technical assistance support could have been used to help address these risks. Sensitivity testing was provided for the financial case, but not for development impact. Finally, the case did not include a logic model or other diagrammatic theory of change, which would have helped to make the assumptions and dependencies underpinning development impact more explicit.
CDC conducted only limited monitoring of development impact for much of the review period, but is now implementing a more systematic approach.
Successive scrutiny reports have concluded that DFID and CDC should do more to capture CDC’s development impact (Box 5). In response, CDC and DFID have repeatedly made commitments to address these concerns. However, progress has been slow.
DFID’s 2017 business case for CDC argued that CDC had outperformed the development impact target that DFID set in the 2012 strategy, and that this demonstrated the organisation’s success in investing responsibly in the most challenging places. We note that this was based on the achieved Development Impact Grid score, which is an ex-ante measure of effectiveness, and did not reflect broader development impacts beyond jobs.
We found significant weaknesses in CDC’s approach to capturing and reporting on the development impact of its investments for most of the review period. For all of the direct investments in our sample, only a very narrow set of results were monitored. Regular reporting included only limited information on development impact, including the number of jobs supported by investee firms (without direct attribution to CDC’s investment, in line with general DFI practice). The reporting was sometimes, but not always, disaggregated by gender and in some cases included CDC’s sector-related metrics. CDC’s quarterly reports on its fund investments (including for the Impact Fund) do not contain information on development impact – instead this is reported on an annual and aggregate basis.
Other weaknesses in CDC’s monitoring included a frequent absence of baselines and targets against which to measure progress (including often for job creation), as well as little external verification. For example, within our sample, CDC made a direct debt investment to support businesses in a country that was recovering from a crisis. It expected to receive data on the financial performance of these businesses to help demonstrate its impact. However, it has subsequently received only one set of data, so has been unable to conclude whether the businesses have grown.
Weak monitoring, combined with insufficient clarity around CDC’s initial development impact expectations, made it difficult for us to assess whether the investments in our sample were on course to deliver their goals. These gaps also suggest that CDC has paid insufficient attention to supporting the achievement of development impact throughout the life of the investments, as part of its portfolio management activities. The lack of monitoring has also limited CDC’s ability to learn (see paragraph 4.140).
Based upon CDC monitoring data and our own interviews, we were able to conclude that nine investments within our sample of 19 were on course to meet the majority of expectations around development impact. These investments met or exceeded their targets for job creation and levels of service provision, although it was difficult (or in some cases too early) to tell whether they were mobilising private capital into their sectors.
We were particularly impressed by Novastar, a fund under the Catalyst Portfolio making investments into a range of early-stage businesses in sectors such as education, healthcare and agri-business, aiming to address unmet demand for goods and services within low-income communities. According to Novastar, more than 2 million poor people, including slum dwellers, have benefited from the businesses within the fund’s investment portfolio, significantly exceeding CDC’s expectations. Another good example was a £38.7 million direct debt investment in the telecommunications sector in Burma, which CDC reports created 327 jobs, 19% more than expected, as well as improving access to services.
However, six investments within our sample had not met the majority of CDC’s impact expectations. Problems included: lower levels of job creation than anticipated, less targeting of poorer people or poorer geographic areas than promised, and smaller effects on the private sector. One fund supported by CDC in India has so far made fewer investments than expected in high-impact sectors and in low-income states within the country, although CDC said that the fund’s future deal pipeline includes such opportunities.
Finally, two of the investments in our sample had such unclear expectations that we could not make a judgment. In the case of one fund investment in Africa, the grid score was within the range of CDC’s expectations, but we found that CDC had not set any expectations for a host of other indicators, including increases in employment and revenue growth in the companies that the fund invested in, or strengthening the market for private sector investment.
We are encouraged to see that CDC’s monitoring of development impact has recently become more systematic. Reports on direct equity investments now have an ‘impact monitoring’ section, which includes coverage of the sector metrics. For all direct investments within the Growth Portfolio, between one and three metrics are now being monitored and reported on. Direct debt investment reports also now describe the key risks to development impact. For example, an investment in the power sector in Africa includes a sector metric on power capacity (measured in megawatts) and considers how progress may be affected by delays in the construction of a power plant. For some Impact Fund investments, additional monitoring ‘deep dives’ are allowing CDC and investees to better understand and improve the impact of the business, by collecting data from the people receiving or using goods and services.
However, there remain important areas for improvement. A CDC ‘work stream’ on impact monitoring was initiated at the beginning of 2017. This planned to establish more rigorous and consistent ways of measuring the development impact of CDC’s investments by the end of that year. As previously noted, the planned thematic metrics for job quality had not been identified at the time of this review. More detailed sector metrics had similarly not been established. CDC now plans to refine these when it develops its sector strategies in 2019.
Within the development impact case that we reviewed, the section on tracking impact listed only a small number of sales and distribution-based metrics – we would have expected to have seen a range of portfolio, sector and thematic metrics, including for direct and indirect employment/livelihood effects, followed by brief details of when and how these are to be monitored, evaluated or modelled. Inclusion of a logic model would also have been helpful in clarifying the range of outputs and outcomes to be measured.
DFID’s latest Annual Review of CDC concluded that CDC’s progress on the monitoring of development impact has been slower than expected. This slow progress means that we are not yet able to assess whether CDC’s plans for improved monitoring of development impact will be implemented systematically across CDC’s investments.
Neither CDC nor DFID is clear about what level of development impact it expects at a portfolio level
In its latest Annual Report, CDC reported on the development impact of its whole portfolio, listing quantitative results on job creation, taxes paid, private finance mobilised and basic sector metrics for five sectors.
Figure 13: Development impact created by CDC’s investee businesses in 2017
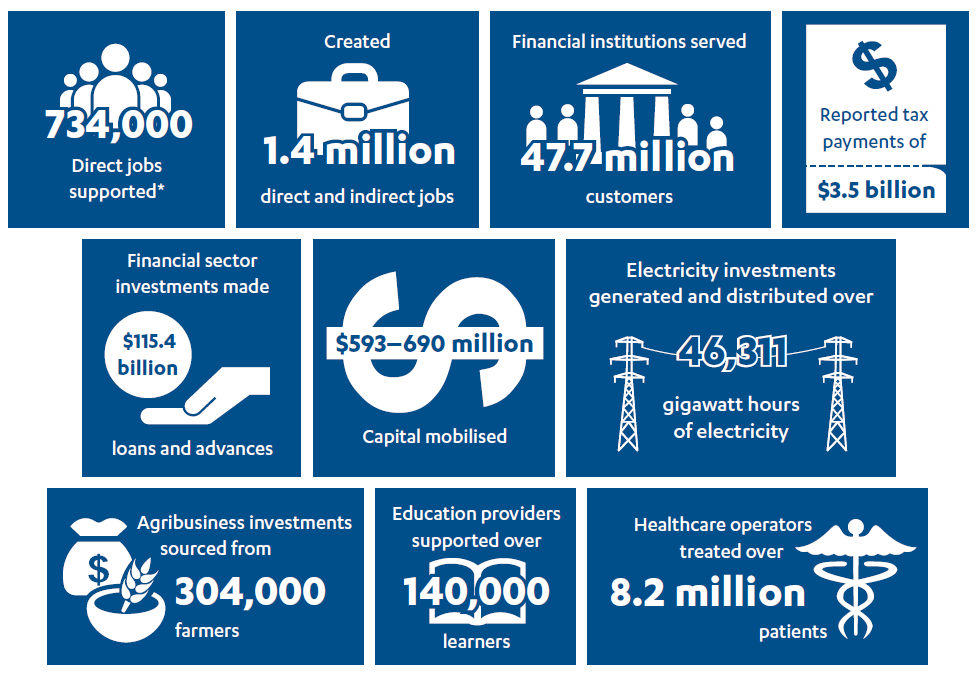
*63,000 were newly created jobs.
Source: Forward with purpose, CDC Group plc Annual Report 2017.
CDC does not claim that all of these development outcomes are attributable to its own investments. Consistent with DFI industry practice, these results represent the aggregate outcomes generated by investee companies. Nonetheless, CDC initiated a work stream in 2017 to develop a clearer position on attribution.
Neither DFID nor CDC set any expectations for their portfolio outcomes, even in gross terms. This means that it is difficult to assess CDC’s effectiveness at an organisational level.
CDC has only recently increased its efforts to understand and drive its mobilisation of private sector investment
In 2009, the Public Accounts Committee recommended that CDC should improve the way that it “measures and reports its effectiveness in mobilising additional investment in deprived areas and markets”. Since then, CDC has reported annually on how much investment it has mobilised directly, alongside its own commitment. In 2017, it began reporting mobilisation statistics using two additional methodologies as well as its own: one developed by the OECD and the other by a consortium of multilateral development banks. Applying these methodologies, CDC reported that it had mobilised $41-48 of private sector capital for every $100 of its own commitments in that year. CDC therefore estimates that the total capital mobilised alongside CDC’s investments in 2017 was $593-690 million. This is down on the amounts CDC estimates that it mobilised in 2015 and 2016.
However, during most of the review period, CDC appears to have not given enough thought to monitoring its mobilisation effects beyond its initial investment, or to reporting on this. Moreover, CDC did not share with us any robust evidence on how it had indirectly helped to mobilise finance over the review period, for example through the wider demonstration effects of investing in a country or sector. The most recent relevant external study considered mobilisation before 2012.
Figure 14: Private sector capital mobilised by year
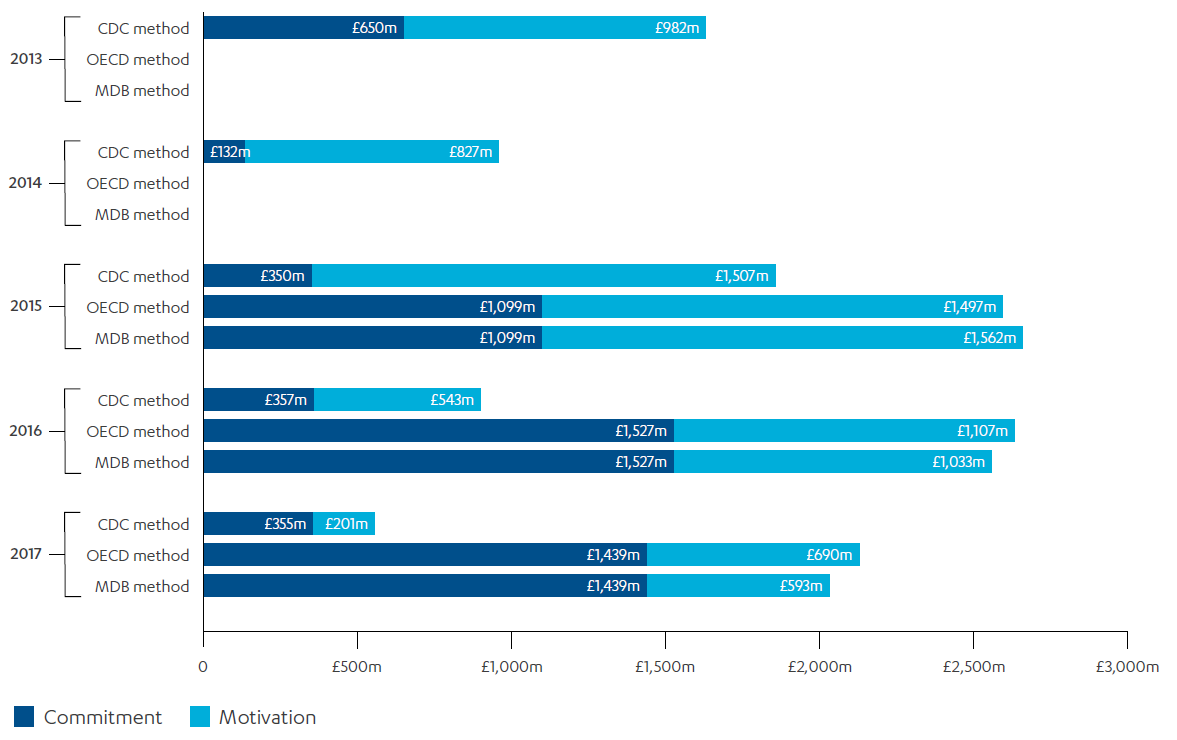
Source: CDC Group plc Annual Review 2017, p. 41.
OECD: Organisation for Economic Co-operation and Development
MDB: Multilateral Development Bank
We heard anecdotal reports of CDC helping to encourage further investment both during and beyond the lifecycle of its investments. In particular, we were told how CDC had worked directly with investee businesses in our sample to improve their proposals to make them more attractive to private investors. For some investments, we also found evidence that CDC’s due diligence and work with the potential investee on ESG issues helped to give confidence to other investors. CDC also hopes to mobilise additional finance indirectly through the positive demonstration effects of it investing in a low-income or fragile state. In our sample of CDC investments, we heard how some fund investments had contributed to establishing and expanding investment markets over the long term, including through supporting first-time fund managers.
CDC is currently working to better understand and drive its wider mobilisation of private sector investment. DFID has commissioned a major longitudinal evaluation of CDC’s mobilisation of capital across markets and sectors, although the survey work had not been started at the time of this review.
CDC does not always take action where there are risks to the development impact of an investment
Impact management is a prominently stated aspect of the Impact Accelerator’s approach to investment. According to CDC, this involves hands-on, proactive management of the impact that investments generate, informed through quantitative and qualitative information gathering. CDC shared its plans with us to roll out this approach across the whole institution, supported by its team of development impact professionals. In practice, we found few examples of portfolio management to enhance development impact within our sample, whether from Impact Accelerator investments or others.
In general, we found that CDC does not do enough to monitor or promote the broader impacts of its investments, or to monitor and mitigate threats to these impacts. One investment in our sample aimed to increase access to affordable housing (defined as lower-middle and middle-income housing) but ended up delivering products for wealthier groups within this range. Having discovered this, CDC agreed that the original plan was not executable and did not seek to influence the investee to build and sell assets to lower-income groups due to risk of financial failure of the fund.
CDC’s success in driving a more developmental strategy for Globeleq provides a good example of how it can support greater development impact during the investment lifecycle (see Box 10).
Box 10: How CDC has used its influence resulting from its majority direct equity stake in Globeleq to drive development impact
Globeleq is the largest private developer, owner and operator of independent power plants in sub-Saharan Africa. It has a generation capacity of more than 1,200 megawatts (MW) in eight locations in Côte d’Ivoire, Cameroon, South Africa, Tanzania and Kenya, with another 2,000 MW under development, including in Sierra Leone and Mozambique.
Developing countries need reliable and affordable electricity to grow businesses, create jobs and improve people’s lives. There is clear evidence that increased power generation is linked with strong growth and employment effects. CDC estimates that Globeleq’s assets support hundreds of thousands of jobs across the countries where it operates.
In 2015, CDC partnered with the Norwegian DFI, Norfund, to take direct ownership of Globeleq, in order to acquire a platform for driving a developmental power strategy across Africa. CDC holds a 70% shareholding in Globeleq, with Norfund holding 30%. Over half ($883 million) of CDC’s capital invested in the infrastructure sector since 2012 was spent on Globeleq.
Since then, CDC and Norfund have driven a new strategy for Globeleq. This strategy has a focus on developing new power generation capacity in Africa to alleviate the shortage of reliable electricity. CDC has managed to influence changes by having two of its senior staff on the Globeleq board, by recruiting a new senior management team who are committed to the new strategic direction, and through financial incentives for Globeleq to work in more difficult country contexts.
CDC is better at assessing and adding value to companies on ESG issues
CDC’s Code of Responsible Investing is widely seen to reflect best practices within the DFI industry. It sets the minimum ESG standards that CDC expects from its investees. Compliance with these standards, as well as any required improvements to meet them, are made a condition of investment. CDC often supports its investees in achieving compliance, for example in relation to industry standards or the impact on local communities. It uses a range of mechanisms to understand their ESG challenges and support improvement. Due diligence assessments made before investment feed into the development of Environmental and Social Action Plans, which CDC monitors. CDC also has ongoing engagement with investees on ESG issues, including through visits to investee locations and training sessions for investee staff.
Investees in our sample were consistently positive about the support they had received from CDC on ESG. 18 of our sample of 19 investments reported that CDC’s investment had contributed to the company making improvements, including strengthening internal staff capacity on ESG and improving their health and safety performance. CDC had also helped the funds it invests in to assess and improve ESG standards among the investee businesses of the funds (see Box 11).
Box 11: CDC’s investment in India Infrastructure Fund II has led to significant ESG improvements
In 2013, CDC invested $200 million into India Infrastructure Fund II, a fund managed by IDFC Alternatives Limited which provides long-term investment for the construction and operation of infrastructure projects throughout India.
CDC’s support to the fund manager on ESG issues has led to clear improvements. The fund manager described CDC as “very responsive”. For example, CDC ESG staff have provided helpful feedback on the fund manager’s draft policies and have worked with fund manager staff to develop better ESG risk management processes. Staff from the fund manager and from portfolio companies have attended CDC ESG training, which the fund manager viewed as useful. CDC was also instrumental in getting the fund manager to hire a social expert and has helped staff responsible for ESG within the fund manager to have a greater voice within the organisation.
In early 2018, safeguarding of aid recipients from sexual exploitation emerged as an area of acute concern across the international development sector, following a number of incidents involving nongovernmental organisations in Haiti. In response, DFID issued new standards on safeguarding to its delivery partners. CDC has subsequently reviewed and strengthened its own internal safeguarding policies and procedures and it plans to make further improvements in its approach to safeguarding with investees, in particular through working to provide more guidance for other investors on safeguarding, and to increase the focus on safeguarding issues in its training programme for investees. CDC also intends to work with other DFIs in an effort to improve safeguarding standards across the industry.
CDC meets industry standards on ESG, which covers safeguarding based upon the IFC’s performance standards. It works with investees to address risks related to the use of child labour, discrimination and exploitation and on other safeguarding issues that have been identified. There are no specific references to sexual exploitation in the Code of Responsible Investing, but much of the language is broad enough to cover this important issue.
CDC told us that when it was notified of a safeguarding incident within a company in which it had invested indirectly through a fund, it worked with that company’s management board to ensure that stronger policies and processes were put in place. CDC recognises, however, that any sexual exploitation of workers and other non-compliance with standards and policies may well be hidden from investors by investee companies and their management. Furthermore, CDC has less direct ability to monitor the investments that it makes through funds (since the fund manager is expected to manage risks on CDC’s behalf). CDC’s current approach is to address this issue as part of its E&S team’s due diligence and subsequent monitoring. More rigorous follow-up evaluation of CDC’s investments, or other third-party monitoring, could help to uncover hidden issues and support efforts to improve safeguarding.
CDC could push harder on achieving greater development impact, while still meeting its financial return targets
Investments in funds in Asia (the vast majority of which are in India) achieve lower average scores on the Development Impact Grid than the rest of CDC’s portfolio, but tend to deliver stronger financial returns. One senior stakeholder in CDC told us that these investments are made to “counterbalance” investments elsewhere with lower predicted returns but greater development impact potential.
We appreciate the importance of achieving financial returns and maintaining a balanced portfolio as CDC moves into riskier markets. However, CDC’s overall financial returns in the review period suggest that it had scope to achieve greater development impact while still meeting its financial return targets. The 2012 – 2017 average return rate on the Growth Portfolio was 10.6% (in GBP), well above the ‘hurdle rate’ of 3.5% agreed with DFID.
Figure 15: CDC’s financial return over the review period
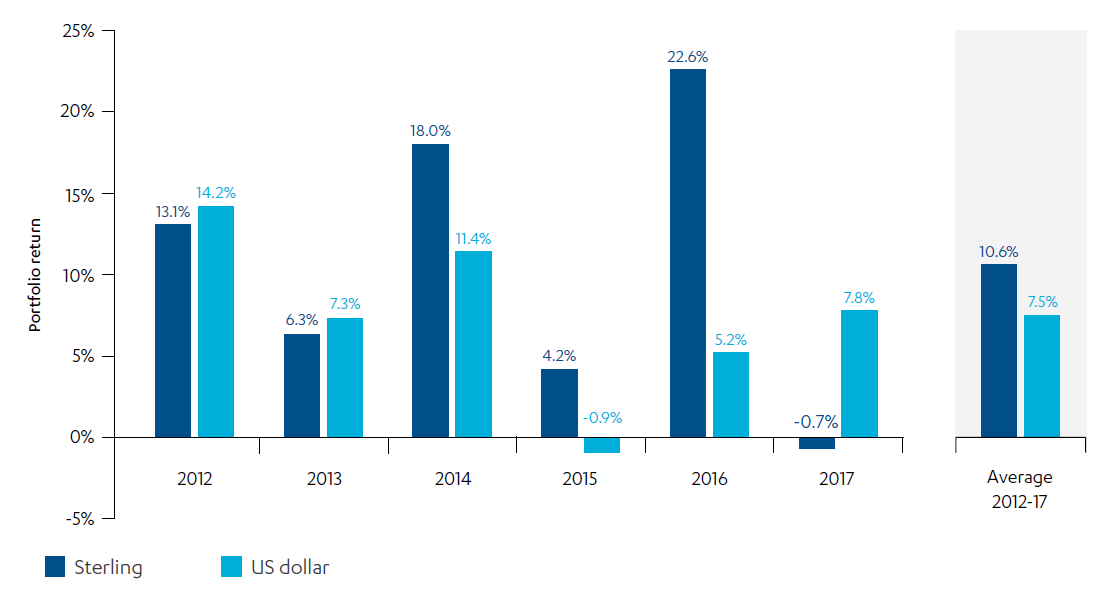
Source: CDC Group plc Annual Review 2017, p. 5.
CDC expects its financial returns to fall as its portfolio becomes increasingly focused on more difficult markets and riskier investments. This is borne out by some of the data. Average returns for new investments in the Growth Portfolio are lower than returns on CDC’s dwindling portfolio of legacy investments made before 2012, and average returns in the Catalyst Portfolio are lower than in the Growth Portfolio. In 2017, following DFID’s reduction of CDC’s overall financial return hurdle to ‘at least break even’ (in GBP), CDC reported a financial return on its entire portfolio (including its Catalyst Portfolio) of 7.3% (in USD) and -1.5% (in GBP), following an increase in the sterling to US dollar exchange rate.
CDC projects significant future losses for investments made under the Catalyst Portfolio, combined with a much lower return on its Growth Portfolio. However, the early scenario planning that ICAI has seen on CDC’s likely future financial returns appears very prudent. The assumptions are based upon data on the realised returns of past investments, as well as early performance of CDC’s Catalyst Portfolio investments (which would be expected to deliver weaker performance in the shorter term), combined with expectations of challenging macroeconomic headwinds.
We believe that there may be some headroom for CDC to give greater priority to development impact, whether by being more ambitious within the Catalyst Portfolio or by driving a greater focus on poverty reduction within its Growth Portfolio. CDC’s expansion of country staff and embedding of development impact professionals within its investment teams should help it to pay more systematic attention to development impact across the lifecycle of its investments, from deal origination through to exit.
Conclusions on effectiveness
CDC has made progress in redirecting its capital towards lower-income and fragile states and its priority sectors. However, there are significant challenges in sourcing impactful investments, particularly in the most difficult markets. Unless it can quickly establish a stronger country presence in Africa, it may struggle to fully meet expectations around scaling up investments in low-income and fragile states over the 2017-21 strategy period as its capital increases.
The investment sourcing and screening stages are crucial for ensuring that CDC’s portfolio of investments achieves maximum development impact. However, for much of the review period, CDC’s procedures for assessing potential impact were less than thorough. CDC has recently enhanced its approach by introducing a development impact case within its Investment Committee papers. Based upon one recent example that we reviewed, areas for improvement remain, including being clearer on the assumptions underpinning development impact.
It is difficult to draw overall conclusions on CDC’s performance in delivering its ambition for development impact, since only a narrow range of indicators were monitored for most of the review period, and expectations around the level of impact to be achieved were often vague. Our assessment was that some of CDC’s investments within our sample had exceeded their anticipated development impacts, while others had not met them.
CDC has made slow progress on measuring actual development impact, whether for individual investments or at the portfolio level. A variety of new initiatives are now attempting to drive improvement.
Once it has invested, CDC is not active enough in understanding and promoting the development impact of its investments. Furthermore, while CDC says that it provides more reporting on mobilisation than its DFI peers, we nevertheless believe that it could strengthen its approach to mobilising other capital. CDC’s success in encouraging ESG improvements suggests that there is considerable potential for it to do more to support enhanced development impact.
We conclude that CDC is not doing enough to maximise the effectiveness of its investments in delivering development impact. While we welcome the recent improvements, including the introduction of development impact cases, it is too early to assess their significance throughout the investment lifecycle. We also believe that many of these improvements could have been made earlier in the review period. We have therefore given CDC an amber-red score for the effectiveness of its investments in low-income and fragile states.
How well does CDC learn and innovate?
CDC is a rapidly growing organisation with an evolving portfolio of investments. In this section we consider whether CDC has suitable systems in place to capture, apply and share learning from its experiences of investing in difficult markets, to help maximise development impact.
CDC has progressively invested more effort in producing learning, but could do more to invest in the most difficult markets
Over the review period, CDC has paid increasing attention to generating learning, using a range of different channels. These include producing bespoke research studies and web resources, and arranging seminars for its staff, investees and the wider investment community.
CDC commissioned research to inform the two major components of its 2012-16 Investment Policy: the creation and use of the Development Impact Grid and diversification into direct investments. This included a 2013 study by McKinsey on the private equity market to inform CDC’s intermediated equity strategy, a 2015 study by PwC on commercial banks to inform its debt strategy, and a 2016 PwC review of the Development Impact Grid scoring and underlying data. This last study concluded that CDC’s existing approach to the grid, and its global target, were broadly sound.
In 2015, CDC set out its procedures for commissioning independent evaluations of development impact and initiated a small number of important learning products linked to its seven priority sectors and the Impact Accelerator. Between 2016 and 2017, CDC commissioned studies on the wider links between energy generation and job creation, which informed its jobs figures, and between SME finance and business growth within its own investments. In 2017, it produced a short learning note on how to build an impact-driven portfolio, drawing on lessons from the Impact Accelerator. More recently, CDC published research on how commercial agriculture can enhance the affordability of protein-rich foods for low-income populations.
We were particularly impressed by the recent research undertaken by Imperial College London to help CDC develop a health impact framework (see Box 12). CDC told us it plans to adopt a similarly rigorous approach in the development of the new strategies and accompanying impact frameworks for its remaining priority sectors.
Box 12: CDC’s health impact framework
CDC worked with Baron Ara Darzi and Imperial College London to investigate how it could maximise its positive impacts within the health sector, asking: “when and how are private sector investments positive for universal health coverage, and when are they negative?”
The research helped CDC to develop a typology of issues to consider when making an investment, covering potential positive and negative impacts on patients (such as on the quality of care) and also for the wider health ‘eco-system’. Through this work, CDC’s Consumer Team (direct equity) has developed a framework which is now applied to new and pre-existing health sector investments to ensure that CDC is making a positive contribution.
CDC is also sharing its learning in this area. The health impact framework report was published on the CDC website in June 2017, academic papers were published in The Lancet and CDC has collaborated with other investors to launch a community of like-minded investors in healthcare, focused on maximising the positive impact of their investments.
At the time of this review, CDC was working on a similar framework for education impact.
We were also impressed by a 2018 study underpinning CDC’s Africa List (Box 13). This provides a further positive example of how CDC can use external evidence to help refine its practices, while introducing more systematic frameworks to help strengthen the generation of its own data in support of learning and improvement.
Box 13: The Africa List
CDC launched the Africa List to find and support future business leaders and entrepreneurs on the African continent and build communities of local business leaders in countries lacking well-established professional networks. The Africa List also helps to increase CDC’s own networks and reach in Africa.
CDC recently completed Driving Impact with Evidence (July 2018, unpublished), a document explaining the theory of change for the Africa List, underpinned by empirical evidence on the power of network effects, and how this will help CDC to learn over time to deliver greater impact. CDC’s Development Impact team was extensively involved in the production of the report.
The report also noted that the metrics previously used to measure the development impact of the Africa List were not fit for purpose and that the new plans for measuring impact were informed by best practice in academic literature.
This positive trajectory is less evident in relation to generating knowledge on how to achieve development impact in the toughest investment markets. Even though CDC prioritises investing in A and B countries and recognises that it faces significant barriers to originating successful deals in these markets, it has not yet tasked experts with gathering systematic evidence on what works in investing in the poorest and most fragile countries and regions, to inform its investment strategy and approach to portfolio management.
CDC’s lack of rigorous monitoring and evaluation for most of the review period has hindered learning on development impact from its own investments
Before 2017, CDC had no strategic plan for monitoring and evaluation or the use of evaluation results to inform investments. Aside from the learning products noted in 4.136, we found few attempts by CDC to investigate the development impact of its own investments or how it can best support investees to maximise their impact, through robust evaluation studies. CDC’s guidelines from 2015 stated that it would adopt a focused approach, initially limiting itself to one or two studies per year. Particularly given the scale of investment by CDC, the lack of robust, external verification for most of the review period, and the missed opportunities for learning as a result, are a serious concern.
We appreciate that, in developing its guidelines, CDC was concerned not to place an undue burden on nascent companies. However, we found that many of the companies in the sample that we visited were keen to discuss their achievements on development impact (for example in relation to jobs and local communities), the challenges and issues that they have had to address, and the potential commercial benefits to their businesses. Many of these investees may therefore have been open to proportionate monitoring and evaluation.
The business case for DFID’s 2017 replenishment of CDC outlined plans for strengthening monitoring and evaluation. This led to the launch of a major new joint programme of evaluation and learning, covering the period from 2017 to 2023 (see Box 14). This programme is intended to provide an overarching framework for CDC’s monitoring and evaluation activities, target its learning priorities (for example by sector) and address knowledge gaps. Both CDC and DFID acknowledge that initiatives under this programme are recent and evolving, and so are still very much work in progress.
Box 14: DFID-CDC evaluation and learning programme: 2017-23 plan
- At least ten deep dives specific to individual investments: building on CDC’s existing evaluation pipeline
- Four to seven large multi-year sectoral studies focused on CDC’s broader development impact above and beyond the impacts being tracked for individual investments
- Investee data monitoring
- Jobs measurement
- Thematic seminars
- A longitudinal evaluation of CDC’s impact on mobilisation and investor perceptions
- A detailed review of the implementation of the 2017-21 strategy
Since the launch of the evaluation and learning programme in 2017, CDC has made progress on improving its processes for investee data monitoring. It now also has plans to conduct brief exit reviews for all direct investments and funds. As the enhanced development cases were only introduced from 2018, it is too early for us to observe whether these changes will improve CDC’s learning from its investments in practice. Based upon the development impact case that we viewed, we believe that the potential for learning could be further enhanced by developing a stronger theory of change against which each investment can be assessed.
CDC also told us that they have made progress in commissioning the series of investment deep dives, which aim to explore how specific investments can achieve impact at scale. These build on CDC’s earlier learning outputs in sectors such as power, SME finance and health. Once complete, the deep dives should provide important learning inputs into CDC’s work to develop new sector strategies. For example, CDC has commissioned a new deep dive into the evidence base for delivering development impact through investing in financial institutions, which would be a useful input to the proposed framework for the financial institutions sector.
CDC’s proposed multi-year sectoral studies can be expected to provide further valuable insights and learnings. However, given that none had been commissioned by the end of 2018, it is unlikely that these studies will have a material impact on investment activities in the current strategy period.
We also understand that a review of the implementation of the 2017-21 strategy is to be carried out at the end of the period. An alternative approach that might provide useful insights earlier in the period would be to conduct a real-time evaluation.
We found less evidence of CDC using learning to inform its decisions and actions on specific investments
CDC says that the learning generated from its investments is shared with its board, the Investment Committee and across CDC investment teams and other internal gatherings of staff.
CDC staff have access to a range of curated learning forums such as ‘air and share’ events (topic-specific talks on CDC investment themes, led by internal and external speakers), a ‘CDC Cinema Showcase’, ‘CDC Forums’ and ‘town halls’, as well as CDC’s internal publications and enhanced intranet resources. These initiatives were strengthened following the launch of the 2017-21 strategic framework, and the appointment of additional staff members to CDC’s communications team.
CDC also told us about a small number of sector-focused working groups, covering for example infrastructure and off-grid solar investments, which bring together investment professionals from each of the product teams. While primarily intended for discussing the investment pipeline and portfolio and identifying opportunities for collaboration, CDC told us that the groups also enable experiences to be shared across CDC.
We welcome the proactive steps that CDC has taken to increase learning opportunities for its staff. However, we found less evidence of structured mechanisms for embedding development impact knowledge within investment decisions and activities. The new healthcare impact framework (see Box 12), which is being applied to both new and existing investments to help improve their development contribution, offers a helpful template for the practical application of learning to CDC’s investment activities.
While we were provided with some examples of informal learning, we found few examples of CDC applying its learning on development impact – whether from its own activities or from external sources – to its own investments. Within our sample, we found positive evidence of CDC using its learning on environmental and social safeguarding issues to inform its selection and management of investments. But we found much less evidence of the practical application of learning on broader development impact issues in our review of relevant Investment Committee papers or in our interviews with CDC staff.
We note that some of CDC’s learning initiatives, and their topics, are quite new. CDC has now published on its website plans for how the data and learning from its evaluation programme will be communicated and applied to the work of different investment teams. The introduction of development impact professionals, working within CDC’s investment teams, provides a further opportunity to improve structured learning. However, suitable knowledge products and knowledge-sharing mechanisms now need to be put in place, covering topics relevant to investing in low-income and fragile states, to maximise the benefits of these new resources.
CDC is a leader in sharing learning on ESG issues and an active contributor to other DFI debates, although it could learn more from its peers
CDC has a strong reputation for sharing learning and encouraging best practice on ESG issues in the DFI community. Its ESG toolkit for fund managers, updated most recently in 2015, is frequently cited by CDC and other DFIs. CDC runs a series of fund manager workshops to encourage better ESG practices across the wider investment industry in developing and emerging markets. CDC has also led on efforts to harmonise DFI reporting for investees on ESG standards, although it admits that it has been difficult to make progress in this area.
In 2018, CDC developed and published a Modern Slavery Guidance note, in collaboration with DFID, the European Bank for Reconstruction and Development, and IFC, and was an anchor sponsor of the Gender-Smart Investing Summit.
CDC supports knowledge sharing in the DFI community across a broad range of other issues, including through convening events and participating in knowledge-sharing platforms. These include the Let’s Work Partnership, Eurodad forums with DFIs,101 the IFC’s working group on DFI Blended Finance and SME Ventures Forum, the Global Impact Investing Network, and various EDFI working groups. A number of external stakeholders told us that CDC is an active participant in these forums, more so than many other DFIs.
More recently, CDC has contributed to a number of initiatives focused on sharing learning on investing in the most difficult markets. In 2017, CDC helped to generate content for the Wilton Park programme ‘Investing for impact: how to make finance work in the most challenging places’. It also contributed case studies to a report from Business Fights Poverty, on unlocking investment to deliver the Sustainable Development Goals in the most challenging places, and presented at its launch.
One sector stakeholder told us they would have liked more engagement from CDC on its new strategy, in order to understand CDC’s approach to investing in the most challenging markets and its rationale for having a separate Catalyst Portfolio. But we also heard positive stories of CDC sharing learning: for instance, CDC shared with other investors the documents and details of the structure that had enabled one of its investees, M-KOPA, a pioneering Kenyan home solar energy firm, to receive loans in its local currency. CDC also said that they have shared learnings on the Impact Fund with other DFIs, in support of their investments in higher-risk/frontier markets.
While CDC is an active contributor to a range of forums and shares learning from its own experiences on development capital, we found less evidence of it taking and applying learning from other DFIs and from other relevant partners to enhance its own strategy, processes and investments.
There has been little joint learning between CDC and DFID, although this looks set to improve
Despite improvements in communication and coordination over the review period, we saw little evidence of joint learning between CDC and DFID, particularly at the country level. Interviews with CDC and DFID staff and with investees and other stakeholders in the countries that we visited provided few examples of joint learning between the two organisations. In particular, we saw little evidence of use by CDC of DFID’s sector expertise or its experience of operating in fragile and conflict-affected states.
We learned of instances where DFID and CDC offices had discussed due diligence issues on investments (for example, CDC worked with DFID and the Foreign and Commonwealth Office on one of our sampled investments in Zimbabwe). However, during the review period there were no systematic processes for CDC and DFID country offices to exchange learning. This represents a missed opportunity for both CDC and DFID.
CDC has told us that this situation is likely to improve significantly with the establishment of a joint evaluation and learning committee, and greater interaction between CDC’s and DFID’s sector and country teams. The appointment of CDC’s sector leads, the development of sector strategies and the strengthening of CDC’s network in Africa all offer substantive opportunities for inter-organisational learning.
CDC could do more to engage with other government departments and with civil society organisations
CDC told us they are increasingly engaged with other UK government departments, and we saw some examples of this on our country visits. However, we think that there is an opportunity for CDC to do better at sharing learning with those departments and cross-government funds involved in mobilising investment in tougher economies, such as the Prosperity Fund.
Since 2017, CDC has also engaged more actively with civil society, for example through briefings and forums on the new capital allocations. Nonetheless, some civil society stakeholders told us that their organisations have felt largely excluded from substantive discussions on CDC strategy and learnings. CDC acknowledges that greater engagement with civil society organisations, particularly those with an economic development focus, could present worthwhile learning opportunities, for example in relation to job quality and equity issues.
Conclusions on learning
CDC has increased its resources for learning during the review period, and there is evidence of thoughtful and rigorous strategic learning initiatives in some priority areas. However, these do not yet add up to a learning and evaluation effort commensurate with CDC’s ambition to deliver greater development impact through investing in difficult markets.
CDC lacks robust evaluation studies of its investments and does not focus enough on gathering systematic learning on how to invest specifically in the most difficult markets. We found limited evidence of CDC applying learning on development impact to investment decisions or to portfolio management.
Significant improvements are now planned, through the joint DFID-CDC evaluation and learning programme launched in 2017. However, some key studies have yet to be commissioned, two years into the new strategy period. Overall, a more dynamic and systematic approach to knowledge capture and sharing is still required, to maximise learning on development impact within CDC.
CDC is a leader among the DFI community in sharing learning around ESG issues, and is expanding this into other priority areas. However, CDC could itself learn more from other DFIs and from civil society organisations, particularly in relation to development impact.
There is scope for both CDC and DFID to benefit from the more systematic and regular sharing of learning between the two organisations. Improvements are planned as part of the development of CDC’s sector strategies and the expansion of its country presence.
While we recognise and welcome the commitment to scaling up evaluation and learning across the organisation, CDC merits an amber-red score for learning. Investment-level monitoring and evaluation have been weak throughout most of the review period, there has been an insufficient focus on learning from the most difficult markets, and we found limited evidence of the application of learning on development impact to investment decisions.
Conclusions and recommendations
Conclusions
CDC has made significant progress in reorienting its portfolio towards low-income and fragile states, as well as towards direct investment, with the intention of driving greater development impact. Its focus on poverty reduction has increased, although the mechanisms through which CDC ensures that its investments reach and benefit the poorest could be more clearly articulated and strengthened.
CDC has significantly scaled up its human resources in support of this work, but has been slow to expand its country network beyond India. CDC has been working to re-establish a country presence in its priority markets since 2013, but by the end of 2017 it only had seven investment staff based in Africa. Failure to establish a credible local presence in its priority markets poses a significant risk to CDC’s ambition to scale up impactful portfolios in challenging geographies.
CDC’s new investments have been concentrated in a small number of larger economies within low-income and fragile countries, as well as in the financial services and power sectors. CDC has faced challenges in finding viable direct investment deals, particularly in Africa.
To facilitate greater risk-taking in pursuit of development impact, DFID has reduced CDC’s financial return targets over the review period. We found that there was room for CDC to strike a more optimal balance between development impact and financial return.
Over the majority of the review period, CDC did not do enough to assess potential development impact when making its investment decisions. As agreed with DFID, CDC was focused on a limited set of metrics including job creation. CDC was often vague or limited in its expectations and did not monitor its performance against broader development impact goals sufficiently. We note that the introduction of development impact cases, in 2018, represents a significant improvement in CDC’s approach, although there is scope to make the assessment of development impact more systematic.
We identified several investments within our sample that did not deliver the development impact that CDC had expected. We also found that CDC was not active enough, once it had invested, in understanding and promoting the impact being achieved by its investees. Additional staff resources are now being recruited to support impact. But these came too late for us to assess whether their efforts will match the progress that CDC has made in promoting good environmental, social and governance standards among its investees.
CDC has introduced a range of learning and knowledge-sharing mechanisms. But during most of the review period, we found limited evidence of CDC applying learning on development impact in the appraisal or management of individual investments. The use of learning has been hampered by the lack of sufficient monitoring and evaluation mechanisms. The new evaluation and learning framework agreed with DFID in 2017 represents a significant improvement, although we note that major sector evaluations under this framework had not been commissioned by the end of 2018. More research and analysis is required on how best to use development finance to achieve impact in the toughest markets. CDC and DFID could also do more to learn from each other, particularly at country level.
In conclusion, DFID’s decision to scale up CDC’s work, and shift its focus towards direct investments and lower-income and fragile countries, placed high demands on CDC, requiring significant changes in its culture, organisation and staffing over a relatively short period of time. CDC has made considerable progress in refocusing the organisation, but there is more to do in a number of important areas, in particular building its in-country presence in Africa, developing sector strategies, strengthening impact management and improving evaluation and applied learning.
Recommendations
We offer a number of recommendations to help CDC increase its development impact in low-income and fragile states.
Recommendation 1
CDC should incorporate a broader range of development impact criteria and indicators into its assessment of investment opportunities, and ensure these are systematically considered in the selection process.
Problem statements
- The Development Impact Grid has helped orientate CDC’s investments towards its priority sectors and geographies. However, its narrow focus on investment difficulty and jobs means that the grid does not necessarily incentivise investment in projects with greatest potential for development impact.
- The Catalyst Portfolio uses a wider range of criteria, including reaching the poorest, additionality of funding and the potential for transformational change, but a set of systematic wider development impact criteria has not been developed for the Growth Portfolio.
- CDC has recently introduced the development impact case to provide a broader view on the potential impact of its investments, alongside the grid score. However, it is currently unclear how these assessments of potential development impacts should be weighted in investment decision-making, relative to other factors.
Recommendation 2
CDC should take a more active role in the management of its investments, using the various channels available to it to promote development impact during their lifetime.
Problem statements
- CDC does not have a systematic approach to enhancing its development impact and does not always make use of the various levers available through its different investment products. In particular, as a shareholder and board member for its direct equity investments, CDC is well placed to influence the strategy and operations of investees.
- We reviewed a recent development impact case to support an investment decision in 2018 and found a need to be clearer at this stage on what actions should be taken to mitigate the risks to development impact.
- Once it has invested, CDC is not always active enough in understanding and promoting development impact during the lifetime of the investment. Many of the investees we spoke to in fact welcomed the opportunity to discuss their achievements and plans in relation to development impact.
- CDC’s processes for assessing development impact and value additionality (and the use of its new technical assistance grant) could be better harmonised to ensure that these functions are mutually supportive in strengthening potential and realised development impact across its investments.
Recommendation 3
CDC should strengthen the monitoring and evaluation of the development impact of its investments and the learning from this, working with DFID to accelerate their joint evaluation and learning programme.
Problem statements
- There is significant variation in how CDC monitors and reports on development impact, as well as a lack of systematic evaluation. This has hampered CDC’s ability to learn from its investments in low-income and fragile states.
- The new development impact cases have the potential to drive better collection of data and learning. Based upon one example that we reviewed, and CDC’s wider plans for measuring development impact, the practical arrangements for monitoring investments could be made clearer. Further common metrics are needed to support consistency.
- In 2017, CDC and DFID launched an enhanced evaluation and learning programme. However, significant strands of evaluation work are not yet under way, and CDC needs clearer mechanisms for ensuring that new learning is applied to investment decision-making processes.
- CDC aims to be pioneering in making large-scale investments in some of the toughest regions, but the new framework does not include plans for specific learning products on investing in difficult markets.
- CDC needs clearer mechanisms for ensuring that new learning is applied to investment decision-making processes.
Recommendation 4
CDC should work more closely and systematically with DFID and other development partners to inform its geographic and sectoral priorities, and build synergies with other UK aid programmes to optimise the value of official development assistance.
Problem statements
- CDC has not yet developed plans or priorities for its activities within individual countries or geographies. These would help to facilitate the prioritisation of its investment activity and coordination with DFID, country governments and other partners, to support transformational growth and attract further investment.
- Although DFID and CDC are starting to work more closely together, particularly at head office, there is potential for greater information sharing and learning at country level.
Recommendation 5
In the presentation of its strategy and reporting to stakeholders, CDC should communicate better its approach to balancing financial risk with development impact opportunity, and the justification for its different investment strategies.
Problem statements
- We accept CDC’s need to balance financial return with achieving development impact but found that CDC is not very transparent about how it achieves this balance, and the trade-offs involved in its decisions, such as investing in some lower-risk countries and sectors.
- External stakeholders were not clear on the differences between CDC’s two different investment strategies, potentially hindering the demonstration objectives for its Catalyst Portfolio and the additionality of its Growth Portfolio.
Recommendation 6
DFID’s business cases for future capital commitments to CDC should be based on stronger evidence of achieved development impact and clear progress on expanding their in-country presence.
Problem statements
- In its latest Annual Report, CDC reported on jobs, taxes, private finance mobilised and very basic impact metrics for five sectors. However, neither DFID nor CDC set any expectations for these outcomes.
- DFID’s business case for its capital injections into CDC did not propose any conditions or targets in relation to development outcomes.
- Outside of India, CDC has been slow to expand its physical presence in its priority markets, despite having made direct investments totalling $1.6 billion in Africa between 2012 and 2017.
- CDC told us that a lack of sufficient country presence is one of its main challenges in sourcing deals at scale in the poorest countries and Indian states.
- A stronger country presence would help with sourcing investments, impact management and monitoring and evaluation. It would also facilitate coordination with DFID and with other development partners.
Annexes
Annex 1 Sampling criteria and approach
The review focuses on CDC’s progress in building its portfolio in difficult investment environments in low-income and fragile countries and its strategies for achieving development impact in such contexts. We used CDC’s own categorisation to identify its most difficult investment locations and selected only A and B countries and states – the two most difficult investment categories – as within the scope of our study. See Figure 16 for how CDC categorises the countries in which it invests.
Figure 16: CDC’s categorisation of countries in which it invests in by investment difficulty
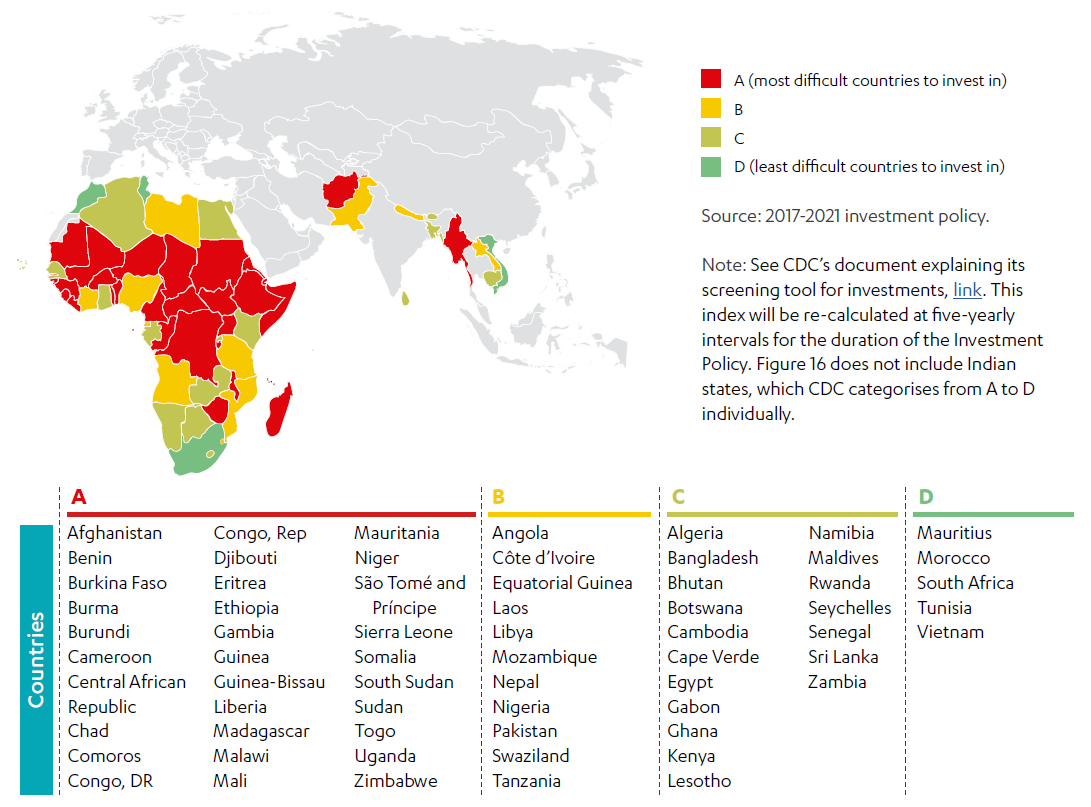
We then selected six out of CDC’s 12 investment teams (as per CDC’s internal structure as of the start of 2018 – See Figure 17), to investigate their approach and operations in a sample of these difficult environments. The six teams were chosen purposively, based on two main criteria, in order to cover:
- CDC investment teams with significant expenditure in difficult markets over the review period
- the major types of investments (direct and indirect) and CDC’s ‘market building’ strategies – the latter being particularly relevant in low-income and fragile countries.
For each of the six investment teams, we then randomly selected a small number of investee funds and companies to review in depth. Our sample consists of 19 new investments in companies, out of the 345 made by CDC in low-income and fragile states since 2012.
The sampled activities are:
- Intermediated Equity: Africa Funds, Asia Funds and Impact Fund
- Direct Equity and Sectors: Financial Institutions and Impact Accelerator
- Debt: Corporate Debt.
Though the sample is small as a proportion of the total number of CDC investments, it provides us with sufficient coverage of (i) the portfolios managed by the investment teams that we have selected and (ii) the three main investment types that CDC uses in low-income and fragile countries: direct investments in companies, indirect investments through intermediary funds, and investments through CDC’s Catalyst Portfolio, which is designed to maximise development impact. Some of the sampled investments were in countries with a stronger CDC footprint, but others were in countries where CDC has less of a presence.
Figure 17: Sampled investment teams within CDC (showing CDC’s investment team structure as of February 2018)
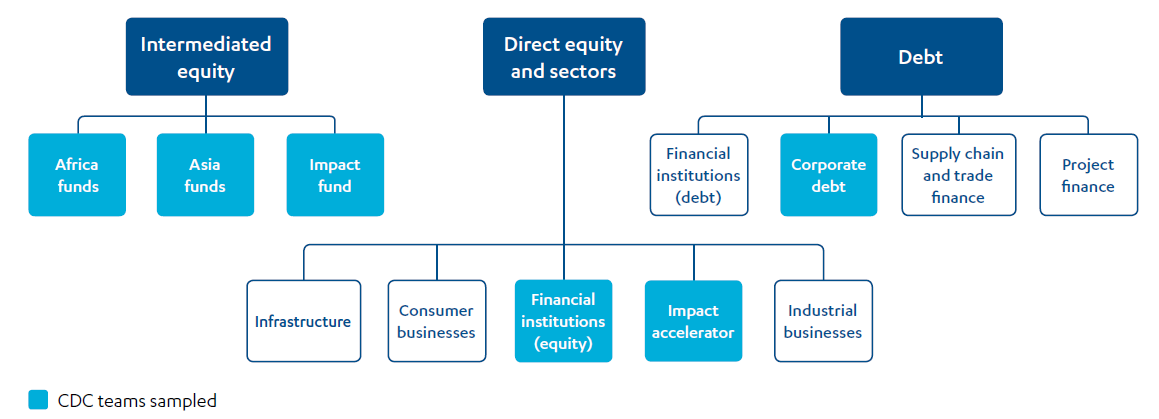
We visited Kenya, Malawi and Nigeria, with a short trip to one location in Tanzania. At the start of the review period (2012) all were A or B countries, although Kenya has since become a C country. Together, they have a reasonably high number of CDC investments across different investment types. These visits gave us the opportunity to visit investees from our sample. For those investments within our sample that were not in the countries we visited, we conducted our assessments remotely.
Figure 18: Overview of different sampling levels

Annex 2 CDC’s investment process
CDC pursues its objectives of supporting the building of businesses throughout Africa and South Asia and making a lasting difference to people’s lives in some of the world’s poorest places through investments. Since CDC’s restructuring in 2012, its investment process has been developed and refined, with the aim of making it more transparent and accountable throughout the investment cycle of sourcing and development, review (screening and due diligence), approval in the Investment Committee, implementation during the life of the investment, and sustainable exit (see Figure 19).
Figure 19: CDC’s investment process